Tubal ectopic pregnancy (unruptured)
















Tubal ectopic pregnancy (or adnexal ectopic pregnancy) is the most common location of an ectopic pregnancy.
Epidemiology
It is the most common type of ectopic by far, accounting for 93-97% of cases.
Pathology
Although the fallopian tube has many anatomical parts, for the purposes of ectopic location it can be divided into :
- ampullary ectopic
- considered the longest segment
- most common site, accounting for ~70%
- isthmic ectopic: ~12%
- fimbrial ectopic: ~11%
Radiographic features
Ultrasound
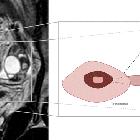
- an adnexal mass that is separate from the ovary is the most common finding and may be seen on in up to 89-100% of cases
- the presence of an adnexal mass becomes more specific for an ectopic pregnancy when it contains a yolk sac or a living embryo or when it moves independently from the ovary
- an extrauterine mass may not be sonographically detected in up to 35% of patients with an ectopic pregnancy
- usually, the corpus luteum is on the same side as ectopic gestational sac ; rupture of the cyst can present with abdominal pain and hemoperitoneum mimicking ectopic rupture
- there may be evidence of a hematosalpinx (a tubal ectopic is the commonest cause for a hematosalpinx)
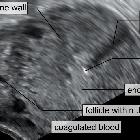
- tubal echogenic ring
- typically a 1-3 cm mass consisting of a 2-4 mm concentric, echogenic rim of tissue surrounding a hypoechoic center
- represents an echogenic ring surrounding an extrauterine gestational sac
- color Doppler interrogation may show peripheral vascularity giving a "ring of fire sign"
- a corpus luteum may have similar color Doppler flow
- there may be evidence of a large hemoperitoneum or large amount of free fluid, especially in cases of rupture
Diagnosis
On transvaginal imaging, findings indicating definitive diagnosis of a tubal ectopic pregnancy :
- extraovarian adnexal mass comprising a gestational sac containing a yolk sac
- extraovarian adnexal mass comprising a gestational sac and fetal pole (with or without cardiac activity)
On transvaginal imaging, findings indicating a high probability of a tubal ectopic pregnancy :
- extraovarian adnexal mass with an empty gestational sac (tubal ring sign or bagel sign), or
- extraovarian heterogeneous adnexal mass (blob sign)
Take into account clinical presentation, serum hCG levels, uterine and adnexal findings.
On transvaginal imaging, findings indicating possible tubal ectopic pregnancy:
- empty uterus
- fluid within the uterine cavity (pseudo sac)
Take into account clinical presentation, serum hCG levels, uterine and adnexal findings.
Treatment and prognosis
Compared to an interstitial ectopic or cervical ectopic, the risk of uncontrollable hemorrhage is fortunately lower. Nonetheless, expedient diagnosis is required.
Management was previously only surgical, with open and then laparoscopic salpingectomy being favored. Salpingotomy (thus preserving the tube) is increasingly performed.
Medical management includes methotrexate (a folate antagonist) either administered systemically or by direct ultrasound-guided injection. After methotrexate therapy, the ectopic pregnancy may show a paradoxical increase in size and vascularity on subsequent imaging even with successful methotrexate.
Increasingly 'conservative' management is being recognized as an option for ectopic pregnancy where rupture has not occurred (i.e no hemoperitoneum) and fetal demise has already taken place.
Complications
Differential diagnosis
- other forms of ectopic pregnancy
- corpus luteum
- may also present as an "adnexal mass" in a patient in whom there is clinical suspicion for ectopic pregnancy and may have similar color Doppler flow
- should be attached to the ovary, whereas a tubal ectopic will slide separately from the ovary with transducer pressure
Siehe auch:
- Extrauteringravidität
- interstitial ectopic pregnancy
- cervical ectopic pregnancy
- Eileiter
- Tubenruptur
- fimbrial ectopic
- haematosalpinx
- ampullary ectopic pregnancy
- isthmic ectopic pregnancy
und weiter:


 Assoziationen und Differentialdiagnosen zu tubal ectopic pregnancy:
Assoziationen und Differentialdiagnosen zu tubal ectopic pregnancy: