transitional cell carcinoma of the bladder





























Transitional cell carcinoma (TCC), also called urothelial cell carcinoma (UCC) of the bladder, is the most common primary neoplasm of the urinary bladder, and bladder TCC is the most common tumor of the entire urinary system.
This article concerns itself with transitional cell carcinomas of the bladder specifically. Related articles include:
- general discussion: transitional cell carcinoma of the urinary tract
- TCCs in other locations:
- other histologies:
Epidemiology
Epidemiology of transitional cell carcinomas of the bladder is similar to those of the rest of the urinary tract: please refer to urinary tract TCC for further details.
Clinical presentation
Hematuria is the most common presenting complaint, which may be macroscopic or microscopic. A tumor located at the vesicoureteric junction may result in ureteral obstruction and hydronephrosis, which may present with flank pain. Additionally, a tumor near the urethral orifice may result in bladder outlet obstruction and urinary retention.
Occasionally patients only present once systemic symptoms of metastatic disease are present.
Diagnosis and local tumor staging are, usually, achieved with cystoscopy and full-thickness biopsy .
Pathology
As is the case elsewhere along the urinary tract, transitional cell carcinomas of the bladder fall into two broad groups :
- superficial: 70-80%
- most are papillary 70%
- high-grade carcinoma in situ: 30% (see TCC grading)
- invasive: 20-30%
Location
The bladder is by far the most common site of transitional cell carcinomas, 50 times more common than TCC of the renal pelvis, and 100 times more common than TCC of the ureter . Bladder TCCs are the most common tumor of the entire urinary tract.
There is a known association of TCCs developing within bladder diverticula, presumably due to urinary stasis which leads to chronic urothelial irritation and potentially the exaggerated exposure to urinary carcinogens .
Risk factors
- cyclophosphamide (a chemotherapy agent) increases the risk of bladder transitional cell carcinoma with a dose-response pattern
- aromatic amines in tobacco smoke
- arylamines used in rubber and plastic manufacturing
- polycyclic aromatic hydrocarbons in industrial combustion processes (such as smelting)
Radiographic features
Imaging of bladder transitional cell carcinomas has a number of roles:
- incidental discovery of the tumor
- tumor staging (see staging of transitional cell carcinoma of the bladder)
- tumor staging of locally advanced masses
- evaluation of distant metastases and nodal status
- surveillance
Ultrasound
Ultrasound has a limited role to play in either diagnosis or staging transitional cell carcinomas of the urinary tract in general.
CT
Bladder transitional cell carcinomas appear as either focal regions of thickening of the bladder wall, or as masses protruding into the bladder lumen, or in advanced cases, extending into adjacent tissues. Care should be taken in assessing bladder wall thickness as this changes with the degree of bladder distension and varies from patient to patient, e.g. patients with bladder outlet obstruction due to benign prostatic hypertrophy. In general, however, asymmetric mural thickening should be viewed with suspicion.
The masses are of soft-tissue attenuation and may be encrusted with small calcifications.
Although unable to distinguish between T1, T2 and T3a (microscopic extravesical spread), CT is able to distinguish T3b tumors (stranding/nodules in perivesical fat) and T4 tumors (direct extension into adjacent structures/loss of normal fat plane) .
Care should be exercised when interpreting stranding or nodularity following transurethral resection or even biopsy, as these changes may be postoperative .
Nodal metastases are common, seen in 30% of T2 tumors and 60% of T3 and T4 tumors .
CT or conventional urography
Urography's primary role is in the assessment of the remainder of the urinary tract for transitional cell carcinomas of the renal pelvis or ureter.
When tumors are large and of papillary morphology, contrast filling the interstices between papillary projections can lead to a dappled appearance referred to as the stipple sign .
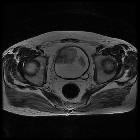
MRI
MRI is superior to other modalities in locally staging the tumor and is in some instances able to distinguish T1 from T2 tumors on T2 weighted images.
- T1: isointense compared to muscle
- T2
- slightly hyperintense compared to muscle
- useful in determining the low signal muscle layer and its discontinuity when muscle wall invasion
- T1 C+ (Gd): shows enhancement
PET
Unfortunately, FDG is excreted into the urine and thus accumulates in the bladder, making it unsuitable for diagnosis of urinary tract tumors. It does have a role to play in the assessment of nodal or distant metastases.
Treatment and prognosis
Treatment is strongly influenced by tumor stage.
Superficial tumors can be treated with local transurethral resection +/- intravesical therapy. Ta tumors can be treated solely by resection. Carcinoma in situ or T1 tumor usually requires both resection and intravesical therapy (bacille Calmette-Guerin (BCG) or chemotherapy, e.g. mitomycin C) .
Invasive tumors require radical cystectomy +/- chemotherapy and/or external beam radiotherapy .
A critical part of the management of patients with TCCs is an awareness of the high rate of recurrence due to field effect on the entire urothelium. Approximately 2-4% of patients with a bladder TCC will go on to develop one or more TCCs of the renal pelvis or ureter .
Superficial tumors (which account for 70-80% of all cases) although having in themselves excellent prognosis, with almost no risk of metastases, have a predilection for recurrence (70% recur within 3 years) and these recurrences are more likely to be invasive. This is especially the case with carcinoma in situ .
Invasive tumors, on the other hand, have poorer prognosis demonstrating both local invasions of perivesical tissues, lymphatic spread to local nodes and eventual haematogenous metastases .
Overall bladder transitional cell carcinomas have a 5-year survival of 82%, contributed mainly by the large proportion of superficial tumors (5-year survival of 94%). Patients with metastatic disease, in contrast, have a poor prognosis (5-year survival of 6%) .
Differential diagnosis
General imaging differential considerations include:
- other bladder tumors / bladder cancers
- squamous cell carcinoma of the bladder
- adenocarcinoma of the bladder
- benign prostatic hypertrophy/prostate cancer
- ureteric jets may simulate a filling defect


 Assoziationen und Differentialdiagnosen zu Transitionalzellkarzinom der Blase:
Assoziationen und Differentialdiagnosen zu Transitionalzellkarzinom der Blase:


