Asbestose






Asbestosis refers to later development of diffuse interstitial fibrosis secondary to asbestos fiber inhalation and should not be confused with other asbestos related diseases.
Epidemiology
Asbestosis typically occurs 10-15 years following the commencement of exposure to asbestos and is dose related . Heavy asbestos exposure is predominantly encountered among men, as most exposures are occupational in the setting of construction, mining, or ship/automotive industries.
Clinical presentation
Clinical presentation is insidious and nonspecific with shortness of breath prompting imaging. Alternatively, the presence of asbestosis may become evident when a patient presents with other asbestos related diseases.
Pathology
Asbestosis is histologically very similar to usual interstitial pneumonia (UIP) with the addition of asbestos bodies .
Radiographic features
Plain radiograph
There are no pathognomonic radiological features specific for asbestosis . Chest radiograph may show irregular opacities with a fine reticular pattern. Additional evidence of asbestos exposure such as calcified or noncalcified pleural plaques may be evident.
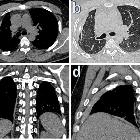
CT
Appearances of asbestosis vary with the duration and severity of the condition. Early manifestations are largely confined to the peripheral region of the lower zones and are subtle. They include:
- centrilobular dot-like opacities: peribronchial fibrosis
- intralobular linear opacities: reticulation
- subpleural lines (often curvilinear)
These changes may be similar in appearance to dependent atelectasis, especially when located posteriorly, and thus supine and prone scans are recommended .
As the fibrosis progresses, a number of more definite findings are seen, which continue to be particularly subpleural and lower lung zone in distribution. They include:
Pleural effusions and pleural plaques are common manifestations of asbestos-related disease.
Mediastinal lymphadenopathy can sometimes be present.
Treatment and prognosis
There is, unfortunately, no proven treatment for asbestosis, and although termination of exposure is, of course, essential, it is usually far too late as many years have invariably already elapsed .
Cessation of smoking is also mandatory as the two are independent and synergistic risk factors for lung cancer .
Progression of disease is variable and appears related to the degree of exposure. Some patients remain stable for many years whereas other progress to end-stage pulmonary fibrosis rapidly . Causes of death include :
- respiratory failure
- cor pulmonale
- asbestos-related malignancy
Differential diagnosis
Consider other causes of pulmonary fibrosis:
- in the absence of pleural plaques or diffuse pleural thickening the differentiation may not be possible on imaging alone
- presence of centrilobular dot-like or branching opacities, subpleural lines and parenchymal bands may be helpful, as they are more common in asbestosis than in idiopathic pulmonary fibrosis
Siehe auch:
- Silikose
- Pleuraplaques
- Pleuramesotheliom
- Pneumonokoniose
- Pleuraplaques bei Asbestose
- retikuläres Muster
- Parenchymband
- subpleural line
- Asbest
- Asbest assoziierte Erkrankungen
- diffuse Pleuraverdickung
und weiter:


 Assoziationen und Differentialdiagnosen zu Asbestose:
Assoziationen und Differentialdiagnosen zu Asbestose: