Dysplastic liver nodules

Qualitative
analysis of small (≤2 cm) regenerative nodules, dysplastic nodules and well-differentiated HCCs with gadoxetic acid MRI. MR scans in a patient with chronic hepatitis, HCV related, and HCC and dysplastic nodule in liver segment V. a-b T2- and T1-weighted fast images show a heterogeneous nodule in liver segment V (arrow). The lesion shows the typical pattern of HCC with enhancement during the arterial phase c) and a wash-out sign on late dynamic phase d). On the late dynamic phase, a lesion near the “hilum-hepatis” is also detectable with loss of signal intensity to the surrounding liver parenchyma (open arrow). e On the fat-suppressed T1 -weighted 3D GRE image obtained during the hepatobiliary phase at 20 min after contrast injection, both lesions are hypointense to the surrounding liver parenchyma. f Histological analysis shows a hepatocellular carcinoma (upper image) and dysplastic nodule (lower image)
A small
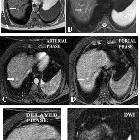
hepatic nodule ( ≤2 cm) in cirrhotic liver: doTriphasic MRI and Diffusion-weighted image help in diagnosis. A 54-year-old male presented with loss of appetite. a An axial unenhanced T1W image shows the right lobe segment IV focal lesion of high signal intensity (arrow). b An axial T2W image shows a lesion of low signal intensity (arrow). c An axial post-contrast arterial phase image showed homogeneous contrast uptake (arrow). d, e An axial portal and delayed images showed persistent contrast enhancement (arrow). f DWI shows the lesion to be of low signal due to non-restricted diffusion (arrow) with an ADC value of 0.7 × 10−3 mm2/s. Suggested MR diagnosis: dysplastic nodule. Biopsy results: high-grade dysplastic nodule
Dysplastic liver nodules are focal nodular regions (≥1 mm) without definite evidence of malignancy.
Epidemiology
They have been found in cirrhotic patients with a prevalence of 14% (size >1.0 cm) to 37% (size >0.5 cm) .
Associations
Pathology
Dysplasia indicates:
- nuclear atypia
- increased fat or glycogen in the cluster of dysplastic cells
Classification
They are broadly divided depending on the presence of cytologic and architectural atypia :
- low-grade: resemble regenerative nodule
- high-grade: resemble well-differentiated hepatocellular carcinoma (HCC)
- atypia is insufficient to establish a diagnosis of HCC
- may exhibit clone-like features
Radiographic features
Ultrasound
Cirrhotic changes are present but the nodules may not be visualized on ultrasound. A few cases have shown hypo- and hyperechoic nodules and the echogenicity relates to the fat content in the nodule.
CT
Usually hypoattenuating, however, they may be iso- or hyperattenuating to the hepatic parenchyma.
- multiphase contrasted images: they may show early arterial uptake but the contrast does not wash out on delayed phase (unlike HCC)
MRI
- T1: although the signal intensity may vary broadly, most of them have high T1 signal
- IP-OOP: shows fat accumulation characterized by signal drop on the out-of-phase sequence
- T2: iso- to hypointense
- DWI: no restricted diffusion
- T1 C+ (Gd)
- high-grade nodules show early contrast enhancement without washout on delayed phase
- T2* C+ (SPIO)
- low-grade nodules appear hypointense
Treatment and prognosis
They are considered premalignant and hence follow-up is necessary. Percutaneous ablation therapy can be considered .
Differential diagnosis
- regenerative nodule
- early hepatocellular carcinoma
- increased T2 signal
- restricted diffusion
- washout on multiphase postcontrast imaging
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu
Assoziationen und Differentialdiagnosen zu 
