Ermüdungsfraktur















































 nicht verwechseln mit: pathologische Fraktur
nicht verwechseln mit: pathologische FrakturFatigue fractures (also known as overuse fractures) are a type of stress fracture due to abnormal stresses on normal bone. They should not be confused with an insufficiency fracture, which occurs due to normal stresses on abnormal bone. Plain radiographs typically demonstrate a linear sclerotic region but have poor sensitivity, especially in early-stage injuries. MRI is the most sensitive and specific modality. Bone scans are sensitive but not specific.
Terminology
Some authors use the term stress fracture synonymously with fatigue fractures, and thus some caution with the term is suggested.
Epidemiology
The demographics are usually young active patients, females more common than males, with specific locations having different demographics in keeping with the associated activity .
Pathology
Fatigue fractures occur when the rate of accumulated microdamage due to a sudden increase in the frequency, intensity, and duration of physical activity is beyond the normal pace of the bony remodeling process.
Accumulation of micro-injuries/microfractures (plastic irreversible deformations) of the normal bone reaching the failing point in which their accumulation exceeds the repair pace/capacity of the bone, hence the gross failure and traumatic fracture ensue. In other words, injury happens faster than healing.
Location
Weight-bearing lower limb fatigue fracture are by far more common. In many cases of lower limb fractures, bilateral abnormalities are present, whereas in the upper limb they are more frequently unilateral and involving the dominant arm:
- pelvis and lower limb (most common)
- medial neck of femur
- compressive forces
- ballet, running, gymnastics
- pubic rami / obturator ring: bowling, gymnastics, stooping
- tibia
- proximal in children
- mid to distal in adults
- calcaneum
- bilateral in up to 27% of cases
- jumping/landing on heels/prolonged standing
- navicular: marching/running
- metatarsals: marching/prolonged standing/ballet
- sesamoid of great toe: prolonged standing
- medial neck of femur
- upper limb
Radiographic features
Early diagnosis is best made with MRI (near 100% sensitive) or bone scan (less specific than MRI) as plain radiographs may appear normal for some time - the sensitivity for early-stage injuries is ~25% (range 15-35%) and late-stage injuries is ~50% (range 30-70%) . CT is not the first neither second line of investigation if stress fatigue fracture is suspected. CT is only indicated in cases which MRI is equivocal due to its higher specificity in detecting fracture lines .
Plain radiograph
Radiographic changes depending on chronicity and cortical-trabecular proportion:
In predominantly cortical bone such as diaphyses findings are as follows in order or progression:
- initially normal
- gray cortex sign: earliest changes, cortical lucency due to microfracture and osteoclastic activity
- cortical thickening: periosteal reaction and endosteal callus formation
- lucent fracture line
In predominantly trabecular bones such as metaphysis of long bones, on the other hand, the first sign would be subtle trabecular blurring and faint sclerosis, followed by a frank sclerotic line. If the fracture extends to the cortex periosteal reactions are also seen.
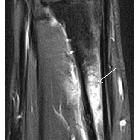
MRI
MRI is as sensitive as bone scanning but is of higher specificity, both in isolating the exact anatomic location and in distinguishing fractures from tumors or infection.
MRI signal characteristics
- T1
- low marrow signal
- very hypointense linear fracture line may be present
- hypointense periosteal/endosteal new bone formation
- T2: high marrow signal with extension into adjacent soft tissues
- T1C+: enhancement can be prominent
Nuclear medicine
There is increased activity at the site of the fracture on bone scans.
Treatment and prognosis
Treatment depends on the location and whether the fracture is complete or incomplete.
Options include conservative management, plaster cast, internal fixation. Most importantly change in behavior to reduce the activity which has lead to the fracture is needed. In some instances, an altered technique may be sufficient to prevent re-occurrence.
Siehe auch:
und weiter:
- Fraktur
- fractures of the extremities - general rules and nomenclature
- Stressfraktur des Schenkelhalses
- Stressfraktur des Femur
- Stressfrakturen des Sakrums
- lytic bone lesion surrounded by marked sclerosis (mnemonic)
- Stressfraktur Kalkaneus
- pubic ramus stress fracture
- co-incidence of spontaneous osteonecrosis and stress fracture
- Stressfraktur der Tibia
- navicular stress fracture
- Stressfraktur proximale Tibia
- longitudinal stress fracture of the tibia
- Bisphosphonattherapie assoziierte Femurfrakturen
- Stressfraktur des Radius
- proximal tibia stress fracture
- stress fractures in the foot and ankle
- subtrochanteric stress fracture
- stress fracture of fibula
- longitudinal stress fracture
- proximale Stressfrakturen Os metatarsale 5


 Assoziationen und Differentialdiagnosen zu Ermüdungsbruch:
Assoziationen und Differentialdiagnosen zu Ermüdungsbruch:

