hemophilia












Hemophilia is an inherited bleeding disorder which is mainly X-linked recessive and therefore occurs almost exclusively in males. There are two main subtypes - hemophilia A (80%) and hemophilia B (20%).
Epidemiology
The incidence of hemophilia A is around 1 in 5000 male births, and the incidence of hemophilia B is around 1 in 25,000-30,000 male births.
Clinical presentation
Most patients present with a bleeding diathesis. In severe cases, patients present during the neonatal or infantile period or with clinically significant bleeding (e.g. cephalohematoma, or post-operative bleeding). In adolescents and adults, hemorrhage typically manifests as bleeding into joints (hemarthrosis) and muscles, whereas bleeding in other more clinically significant sites such as intracranially or gastrointestinal are relatively uncommon. The types of hemophilia are impossible to delineate clinically .
Complications
- haemophilic arthropathy
- osteopaenia and osteoporosis
- transfusion-related diseases:
- HIV
- hepatitis C
- Creutzfeldt-Jacob disease (CJD) (very rare)
Pathology
The main forms of hemophilia are inheritable X-linked recessive diseases , with ~70% considered familial and ~30% considered sporadic . Generally, severity is graded depending on baseline factor activity:
- mild: factor activity 6-40% of normal
- moderate: factor activity 1-5% of normal
- severe: factor activity <1% of normal
Hemophilia A
- ~80% of cases
- F8 gene mutation, on the long-arm of the X-chromosome
- inherited as an X-linked recessive condition
- coagulation factor VIII deficiency or absence
Hemophilia B
- a.k.a. Christmas disease
- ~20% of cases
- F9 gene mutation, on the long-arm of the X-chromosome
- inherited as an X-linked recessive condition
- coagulation factor IX deficiency or absence
Hemophilia C
- a.k.a. Rosenthal syndrome
- <1% of cases,
- most common in Ashkenazi Jewish population
- F11 gene mutation, on the long-arm of chromosome 4
- inherited as an autosomal recessive or dominant condition
- coagulation factor XI deficiency or absence
Radiographic features
The hallmark of the disease is hemorrhage, particularly into joints and/or soft-tissue, with several radiological consequences:
- haemophilic arthropathy occurring in almost all individuals
- haemophilic pseudotumor occurring in ~2%
- soft tissue hematoma formation may lead to contractures
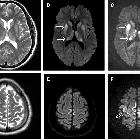
- serious life-threatening hemorrhage (intracranial, thoracic, abdominal)
Treatment and prognosis
Treatment depends on the type, general severity, current clinical state, and can be delivered episodically or prophylactically. Options for treatment include factor products (plasma-derived or recombinant), or novel medications such as emicizumab .
Prognosis depends on the severity and on the presence or absence of transfusion-related disease. Complications from HIV and cirrhosis are leading causes of death. Life expectancy in those without HIV is ~62 years .
- ~15 times increased risk death from intracranial hemorrhage (~1/3 of all deaths)
- ~50 times increased risk death from non-intracranial hemorrhage
See also
Siehe auch:
- Intrakranielle Blutung
- Creutzfeldt-Jakob-Krankheit
- hämophile Arthropathie
- hämophiler Pseudotumor
- muskuloskelettale Komplikationen der Hämophilie
und weiter:
- idiopathische kindliche Hüftkopfnekrose
- Hüftkopfnekrose
- Chondrokalzinose
- siderotic synovitis
- macrodystrophia lipomatosa
- Kalziumpyrophosphat-Ablagerungskrankheit
- chondrocalcinosis (mnemonic)
- premature closure of a growth plate
- Hämophilie
- multiple benign lucent bone lesions (mnemonic)
- differential diagnosis of epiphyseal overgrowth
- Arthritis Knie
- Hämangiom-Thrombozytopenie-Syndrom
- haemophilia: skeletal manifestations


 Assoziationen und Differentialdiagnosen zu Hämophilie:
Assoziationen und Differentialdiagnosen zu Hämophilie: