idiopathic granulomatous mastitis














Idiopathic granulomatous mastitis is a very rare breast inflammatory disease of unknown origin that can clinically mimic carcinoma of the breast.
Clinical presentation
The condition generally manifests as a distinct, firm to hard mass that may involve any part of the breast. The subareolar regions may be relatively spared. The relationship of granulomatous mastitis to pregnancy or lactation has been strongly emphasized because this disease entity typically affects younger women, usually within 6 years of pregnancy. Reactive lymph nodes may be present in up to 15% of cases.
Pathology
Immunologic factors have been postulated as possible causes; however, the absence of vasculitis or of a prominent lymphocytic component in pathologic specimens favors against this hypothesis.
The diagnosis of idiopathic granulomatous mastitis is based on exclusion, since it depends on the demonstration of a particular histologic pattern combined with the exclusion of other granulomatous reactions such as:
- especially tuberculosis
- sarcoidosis
- granulomatosis with polyangiitis
- fungal infections
- and those other benign inflammatory disorders found in association with carcinomas
At pathologic analysis, idiopathic granulomatous mastitis manifests as a non-caseating, non-vasculitic granulomatous inflammatory reaction centered on lobules. Fat necrosis, abscess formation, and fibrosis are commonly associated end-stage features that can disrupt the normal lobular anatomy.
Radiographic features
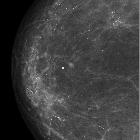
Mammography
Mammographic features can be variable, ranging from normal findings in patients with dense breasts to masses with benign or malignant features and focal asymmetric density. The most common mammographic appearance of the lesion is an asymmetrically increased density, which is not characteristic for this entity .
Breast ultrasound
Sonographic patterns of the disease are also varied and appear to relate to the histologic features. Findings include a mass-like appearance, tubular/nodular hypoechoic structures and focal decreased parenchymal echogenicity with acoustic shadowing.
Breast MRI
On MRI, the most frequent finding is focal or diffuse asymmetrical signal intensity changes without significant mass effect. Nodular lesions can also be seen .
- T1: regions tends to be hypointense
- T2: regions tend to be hyperintense
- dynamic contrast-enhanced MRI: can show mass-like enhancement, ring-like enhancement, and/or nodular enhancement while time-intensity curves can differ from patient to patient and from lesion to lesion
Treatment and prognosis
The prognosis is usually good, although local recurrence has been reported. Primary treatment usually comprises of excisional biopsy. Corticosteroid therapy has also proved effective.
Siehe auch:
- Tuberkulose
- Verkalkungen in der Mammographie
- Sarkoidose
- Granulomatose mit Polyangiitis
- Mastitis
- duktales in situ Karzinom der Mamma
- chronische abakterielle Mastitis
- Neoplasien der Mamma
- granulomatöse Mastitiden allgemein
und weiter:


 Assoziationen und Differentialdiagnosen zu idiopathische granulomatöse Mastitis:
Assoziationen und Differentialdiagnosen zu idiopathische granulomatöse Mastitis: