Kraniosynostose
























Craniosynostosis refers to the premature closure of the cranial sutures. The skull shape then undergoes characteristic changes depending on which suture(s) close early.
Epidemiology
There is a 3:1 male predominance with an overall incidence of 1 in 2000-2500. 8% of cases are syndromic or familial.
Pathology
Primary forms are either sporadic or familial. Secondary craniosynostosis occurs in relation to a variety of causes:
- endocrine disorders
- hyperthyroidism
- hypophosphatemia
- vitamin D deficiency
- hypercalcemia
- hematologic disorders causing bone marrow hyperplasia
- sickle cell
- thalassemia
- inadequate brain growth
- microcephaly
- shunted hydrocephalus
Ages of normal sutural/fontanelle closure
- metopic: 3-9 months
- anterior fontanelle: 18-24 months
- sphenosquamosal: 6-10 years
- sphenofrontal: approximately 15 years
- occipitomastoid: approximately 16 years
- sagittal: approximately 22 years
- coronal: approximately 24 years
- lambdoid: approximately 26 years
- squamosal: approximately 60 years
Types
- brachycephaly: bicoronal and/or bilambdoid sutures
- scaphocephaly/dolichocephaly: sagittal suture
- plagiocephaly: unilateral coronal and lambdoid sutures
- frontal plagiocephaly: unilateral coronal suture
- occipital plagiocephaly: unilateral lambdoid suture
- trigonocephaly: metopic suture
- pachycephaly: lambdoid suture
- oxycephaly/turricephaly: sagittal, coronal and lambdoid sutures (Tower like skull)
- cloverleaf skull/Kleeblattschadel: intrauterine sagittal, coronal, lambdoid sutures (most severe)
- harlequin eye: ipsilateral coronal suture
- progressive postnatal pansynostosis: rare form of craniosynostosis which involves late (postnatal) fusion of all cranial sutures
The sagittal suture is most commonly involved (≈50%), where the lateral growth of the skull is arrested while anteroposterior growth continues, producing a narrowly elongated skull known as scaphocephaly (meaning boat-shaped) or dolichocephaly (from the ancient Greek for long, δολιχός: dolichos).
The next most common sutures in terms of involvement are:
- coronal (~20%)
- lambdoid (~5%)
- metopic (~5%)
Associations
Most occur as isolated anomalies but syndromic associations can be seen in a small proportion of cases (~10%):
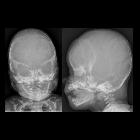
Radiographic features
Restriction of skull growth is perpendicular to the affected suture line. Characteristic dysmorphic head shapes are associated with each type of craniosynostosis.
Ultrasound
Ultrasound may be useful in subtle cases. General features include:
- sutures are normally hypoechoic
- there may be a loss of normal decreased echogenicity in the region of the fusion
- lack of suture patency
- ridging of the sutures
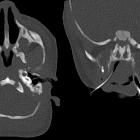
CT
CT with 3D image reformations is the best modality used for evaluation of sutures .
Treatment and prognosis
Treatment is often with a cranioplasty. Abnormal intracranial pressure may affect neurocognition.
Siehe auch:
- Dolichocephalie
- Pfeiffer-Syndrom
- Kleeblattschädel
- Choanalatresie
- Apert-Syndrom
- Crouzon-Syndrom
- acrocephalosyndactyly
- Impressiones digitatae
- Carpenter syndrome
- Brachyzephalie
- kranio-fronto-nasale Dysplasie
- Baller-Gerold-Syndrom
- Muenke-Syndrom
- Plagiozephalie
- Trigonocephalie
- persistierende Sutura frontalis mediana
- oxycephaly / turricephaly
- harlequin eye
und weiter:
- Hypotelorismus
- acrocephalopolysyndactyly
- acrocephalopolysyndactyly type II
- Saethre-Chotzen-Syndrom
- Sutura sagittalis
- Kupferkesselschädel
- Klassifikation Osteogenesis imperfecta
- Osteoglophone Dysplasie
- CAP-Syndrom
- Dzierzynsky-Syndrom
- Frank-ter Haar-Syndrom
- brachycephaly (bicoronal synostosis)
- Pseudoaminopterin-Syndrom
- high-head syndrome
- coronal synostosis
- Synostose der Sutura sagittalis
- brachycephaly (bi-coronal and bi-lambdoid synostosis)
- unilateral coronal suture synostosis
- unilateral coronal synostosis
- Suturen


 Assoziationen und Differentialdiagnosen zu Kraniosynostose:
Assoziationen und Differentialdiagnosen zu Kraniosynostose: