Leberblutung





























The liver is one of the most frequently damaged organs in blunt trauma, and liver trauma is associated with a significant mortality rate.
Epidemiology
In blunt abdominal trauma, the liver is injured ~5% (range 1-10%) of the time .
Clinical presentation
Patients can present with right upper quadrant pain, right shoulder tip pain (from diaphragmatic irritation), hypotension, and shock .
Pathology
Etiology
The mechanism for liver trauma can be from blunt (e.g. motor vehicle collision, fall, direct blow, etc.) or penetrating trauma (e.g. gunshot, stabbing). It can also be iatrogenic (e.g. percutaneous liver biopsy).
Types
Most (~80%) of liver injuries are minor (grades I to III). There is a range of injuries:
- laceration (most common)
- hematoma - subcapsular or intraparenchymal
- active hemorrhage
- major hepatic vein injury
- arteriovenous (AV) fistula
- bile duct injury
Associations
Approximately 80% of liver injuries are associated with other abdominal injuries .
Within the liver:
- lacerations that involve a hepatic vein are associated with increased risk of arterial injury and need for operative management
- although not an injury, periportal edema can be seen associated with liver injuries as patients with higher-grade injuries will have received aggressive fluid resuscitation
- lacerations that extend to the porta hepatis increase the risk of bile duct injuries, particularly delayed biliary complications
- bile duct injuries are more common in :
- higher grade injuries
- central injuries, that is injuries that are close to the IVC
- penetrating trauma, compared with blunt trauma
Outside the liver (known as secondary signs):
- lacerations that extend to the bare area can be associated with a retroperitoneal hematoma or an adrenal hemorrhage
- right lower lobe pulmonary contusion/laceration
- right-sided rib fractures
- transverse process fractures
- hemo/pneumothorax
- right kidney injury
Markers
Elevated liver transaminases (ALT/AST) are 100% specific and ~93% sensitive in predicting liver injuries .
Radiographic features
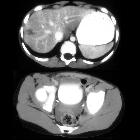
CT
CT is the investigation of choice for evaluating liver trauma. It is ~95% sensitive and 99% specific for detecting liver injuries .
- lacerations appear as irregular linear/branching areas of hypoattenuation
- hematomas appear as a hypodensity between the liver and its capsule (and can be differentiated from intra-peritoneal hematoma as these distort the liver architecture) or can be intraparenchymal
- acute hematomas/hemorrhage are typically hyperdense (40-60HU) compared to normal liver parenchyma
- muscular diaphragmatic slips may simulate a peripheral laceration but are smoother, non-branching and of muscle density when compared to a laceration
If the liver is diffusely hypoattenuating, such as seen in steatosis, lacerations and hematomata may be more subtle to diagnose . Secondary signs should help.
See the main article liver injury grading for more details.
Hepatic scintigraphy
Scintigraphy, such as that using Tc-99m mebrofenin or disofenin, is the most commonly used test for the diagnosis of bile leaks . A contained leak will demonstrate an extrabiliary focus of radiotracer which remains stable in size and morphology during all the phases of the study. A free intraperitoneal bile leak will demonstrate an extraluminal collection of radiotracer in the peritoneal cavity that varies or increases in time .
Differential diagnosis
Several mimics of liver lacerations and hematomata exist, and include :
- focal fat infiltration
- unenhanced aberrant portal or hepatic veins
- congenital fissures and clefts: typically fat density, and in usually locations
- diaphragmatic slips or eventration: identifiable on coronal images
- pre-existing liver lesions
- cysts
- hemangioma
Treatment and prognosis
Most (>80%) of liver injuries can be treated non-surgically, and in blunt trauma relies on hemodynamic stability rather than a grade of injury . There is a significant mortality rate of ~8% (range 4.1-11.7%) associated with liver trauma . Complications are reported in ~20% of cases of non-operatively treated liver trauma :
- abdominal compartment syndrome
- bile duct injury leading to bile peritonitis or biloma
- delayed hemorrhage
- intra-abdominal abscess formation
- acute acalculous cholecystitis
Siehe auch:
- subkapsuläres Leberhämatom
- AAST liver injury scale
- Leberkontusion
- stumpfes Bauchtrauma
- Leberhämatom
- Parenchymeinblutungen der Leber
- intraabdominelle Blutungen
und weiter:


 Assoziationen und Differentialdiagnosen zu Leberblutung:
Assoziationen und Differentialdiagnosen zu Leberblutung:

