madelung deformity










 nicht verwechseln mit:
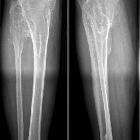
nicht verwechseln mit: Madelung deformity refers to bowing of the radial shaft with increased interosseous space and dorsal subluxation of the distal radioulnar joint. This deformity is due to premature closure or defective development of the ulnar third of the distal epiphysis of the radius.
Madelung deformity can be bilateral in 50-66% of patients. It often occurs as a rare congenital deformity and does not usually manifest until 10-14 years of age. It may also be seen as an acquired consequence of trauma to the growth plate, e.g. Salter-Harris fracture (type V). The congenital form has autosomal dominant inheritance with variable penetrance.
Terminology
Madelung deformity should not be confused with Madelung-Launois-Bensaude syndrome, also referred to as Madelung disease, which is characterized by lipomatous accumulation in the subcutaneous regions of the neck, upper thorax, and upper limbs .
Epidemiology
The abnormality is more common in females by a 4:1 ratio .
Clinical presentation
Most non-traumatic cases of Madelung deformity present with progressive deformity during late childhood or early adolescence . The presentation is with deformity, decreased grip strength, and often with pain in the wrist relating to ulnocarpal impaction .
Pathology
The common mechanism for all causes of Madelung deformity is premature closure or failure of development of the ulnar side of the distal radial physis. Arrest of epiphyseal growth of the medial and volar (anterior) portions of the distal radius leads to shortening of the radius and relative overgrowth of the ulna. The underlying cause of this is unclear, with possibilities including :
- vascular insufficiency
- trauma
- infection (osteomyelitis)
- muscular disorders
Associations
- Leri-Weill syndrome: an autosomal dominant dyschondrosteosis (a form of mesomelic dwarfism)
- Turner syndrome: affects wrists and hands with osteopenia, metacarpal bones shortening (especially 4), and decreased carpal angles, which resemble Madelung deformities (usually bilateral)
- Madelung dyschondrosteosis
- gonadal dysgenesis
- nail-patella syndrome
- diaphyseal aclasis (hereditary multiple exostoses)
- Hurler mucopolysaccharidosis
- achondroplasia
- Ollier disease
Radiographic features
The deformity is characterized by:
- dorsal and radial bowing of the radius
- increased interosseous space
- exaggerated palmar (up to 35°) and ulnar tilt (up to 60°) of the radiocarpal articulation
- failure of ossification of the ulnar side of the distal radial epiphysis
- exaggerated radial inclination
- decreased carpal angle below 118° (normal ranges from 118° to 139°)
- carpal subluxation in a palmar and ulnar direction
- lunate is gradually forced to the apex of the V-shaped radio-ulnar-carpal joint
- “V-shaped” proximal carpal row = herniated proximal carpal row.
- dorsal subluxation of the distal radio-ulnar joint
- positive ulnar variance
- wedging of the carpus between the radius and ulna
Treatment and prognosis
Many treatments have been proposed and tried, often with limited success. Conservative measures tend to be ineffective. Surgical options include :
- radial epiphysiodesis
- radial corrective osteotomy
- radial physiolysis
- ulnar epiphysiodesis
- excision of the distal ulnar
- ulnar shortening osteotomy
History and etymology
Madelung deformity was first described in 1878 by Otto Wilhelm Madelung (1846-1926), a German surgeon .
Differential diagnosis
- trauma
- distal radius and ulnar trauma can cause Madelung deformity when the distal radius' medial joint fuses with the ulna while the lateral joint space continues to grow. This is seen especially when the physis is still open.
- infection
- can cause abnormal fusion of the distal radial and ulnar growth plates, The Madelung deformity occurs when the distal radius medial joint fuses with the ulna while the lateral joint space continues to grow.
- Turner syndrome
- in females with a 45/XO.
- other hand findings are osteopenia, metacarpal shortening (especially 4th metacarpal), and decreased carpal angles which resemble Madelung deformities
- usually bilateral
- skeletal dysplasias
- Ollier disease
- diaphyseal aclasis (hereditary multiple exostoses)
- Mucopolysaccharidoses
- usually bilateral
Siehe auch:
- Osteomyelitis
- Achondroplasie
- Ollier-Syndrom
- Multiple kartilaginäre Exostosen
- Ulnaminusvariante
- Turner-Syndrom
- ulnokarpale Impaktation
- Mukopolysaccharidose Typ I-H
- gonadal dysgenesis
- Nagel-Patella-Syndrom
- Madelung dyschondro-osteosis
- madelung deformity associations (mnemonic)
- Madelung-Krankheit
- Dyschondrosteose Léri Weill
und weiter:


 Assoziationen und Differentialdiagnosen zu Madelung-Deformität:
Assoziationen und Differentialdiagnosen zu Madelung-Deformität: