Osteoid-Osteom Schenkelhals




Osteoid-Osteom Schenkelhals
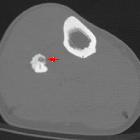
Osteoid-Osteom Radiopaedia • CC-by-nc-sa 3.0 • de
Osteoid osteomas are benign bone-forming tumors that typically occur in children (particularly adolescents). They have a characteristic lucent nidus less than 1.5 or 2 cm and surrounding osteosclerotic reaction, which classically causes night pain that is relieved by the use of salicylate analgesia, e.g. aspirin.
Epidemiology
Osteoid osteomas are usually found in children, adolescents, and young adults, between the ages of 10 and 35 years .
They account for ~10% of all benign bone lesions and there is a male predilection (M:F 2-4:1) .
Clinical presentation
Classically patients present with nocturnal pain and is relieved by salicylates (e.g. aspirin).
When in the spine they are a classic cause of painful scoliosis, concave on the side of lesion. This typical presentation is seen in over 75% of cases .
Soft tissue swelling may occur (see case 4) and if close to a growth plate, accelerated growth may be evident , presumably related to hyperemia.
When the lesion is intracapsular, the presentation is more atypical, and more likely mimics inflammatory arthropathy or synovitis. Joint effusion is often present .
Pathology
An osteoid osteoma is composed of three concentric parts :
- meshwork of dilated vessels, osteoblasts, osteoid, and woven bone
- may have a central region of mineralization
The nidus releases prostaglandins (via the enzymes cyclo-oxygenase-1 and cyclo-oxygenase-2) which in turn result in pain .
Location
Most osteoid osteomas occur in long tubular bones of the limbs (especially the proximal femur), but any bone may be involved.
- long bones of the limbs: ~65-80%
- femur most common (especially neck of femur)
- mid-tibial diaphysis common also
- phalanges: ~20%
- vertebrae: ~10%, predominantly posterior elements
- lumbar: 59%
- cervical: 27%
- thoracic: 12%
- sacrum: 2%
Furthermore, osteoid osteomas are usually cortical lesions but they can occur anywhere within the bone including medullary, subperiosteal (most commonly in the talus), and intracapsular .
Radiographic features
It is important to remember that the sclerosis is reactive and does not represent the lesion itself. The nidus is usually <2 cm in diameter, and is typically ovoid. It may have a central region of mineralization .
Plain radiograph
May be normal or may show a solid periosteal reaction with cortical thickening. The nidus is sometimes visible as a well-circumscribed lucent region, occasionally with a central sclerotic dot.
CT
CT is excellent at characterizing the lesion and is the modality of choice. It typically shows a focally lucent nidus within surrounding sclerotic reactive bone. A central sclerotic dot may also be seen.
Nuclear medicine
Skeletal scintigraphy will show typical focal uptake and at times will show a double density sign (also known as the less catchy hotter spot within hot area sign) which if present is highly specific and helpful in distinguishing it from osteomyelitis. The central focus showing intense uptake within a surrounding lower - but nonetheless increased - uptake rim.
Ultrasound
On ultrasound, focal cortical irregularity with adjacent hypoechoic synovitis may be present at the site of intra-articular lesions. The nidus can show hypoechogenicity with posterior acoustic enhancement. Ultrasound may be able to identify the nidus as a hypervascular nidus on Doppler examination .
MRI
Although MRI is sensitive, it is non-specific and is often unable to identify the nidus. The hyperemia and resultant bone marrow edema pattern may result in the scans being misinterpreted as representing aggressive pathology .
The signal intensity of the nidus is variable on all sequences as is the degree of contrast enhancement .
Treatment and prognosis
The lesion is benign and treatment has traditionally been with surgical resection. Historically, this has, on occasion, been difficult because of the inherent inability to locate the nidus during surgery . However, percutaneous radiofrequency ablation under CT guidance is being used with increasing frequency .
There is growing evidence, that osteoid osteoma naturally resolves spontaneously with time and can be treated conservatively with NSAIDs in certain groups of patients . The average time to resolution is 33 months.
Differential diagnosis
General imaging differential considerations include:
- osteomyelitis (e.g. Brodie abscess): bone scan demonstrates central area of reduced uptake representing an avascular area of purulent material
- osteoblastoma: >1.5-2 cm in size
- stress fracture
- cortical desmoid
- osteochondroma
- osteosarcoma
- enostosis (bone island)
- localized cortical thickening
- intracortical hemangioma
- reactive sclerosis around an osteolytic lesion
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Osteoid-Osteom Schenkelhals:
Assoziationen und Differentialdiagnosen zu Osteoid-Osteom Schenkelhals: