pancreatic lymphoma





Pancreatic lymphoma is most commonly a B-cell sub-type of non-Hodgkin lymphoma.
Epidemiology
Pancreatic lymphoma is typically seen in middle-aged patients with a mean age of around 55 years old and is more common in immunocompromised patients.
Clinical presentation
Symptoms are often non-specific but may include :
- abdominal pain ~ 85%
- mass ~ 60%
- weight loss ~ 50%
- obstructive jaundice ~ 40% of cases
- acute pancreatitis 10%
The classic B-symptoms of non-Hodgkin lymphoma (e.g. fever, chills, night sweats) are present in only 2% of cases .
Pathology
Etiology
It is classified as either primary or secondary:
- primary pancreatic lymphoma is a rare extranodal manifestation of any histopathologic subtype of B-cell non-Hodgkin's lymphoma, representing <2% of extranodal lymphomas and 0.5% of pancreatic tumors
- secondary lymphoma: found in 30% of non-Hodgkin lymphoma patients with widespread disease, it is the dominant form and is the result of direct extension from peripancreatic lymphadenopathy
Location
Two morphologic patterns of pancreatic lymphoma are recognized :
- focal form: occurs in the pancreatic head in 80% of cases and has a mean size of 8 cm
- diffuse form: infiltrative, leading to glandular enlargement and poor definition, features that can simulate the appearance of acute pancreatitis
Radiographic features
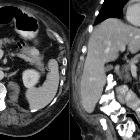
CT
- minimal enhancement
- peripancreatic lymph node enlargement
- it typically has uniform low attenuation
- diffuse enlargement (diffuse form) may simulate acute pancreatitis
- encasement of the peripancreatic vessels may occur; vascular invasion is less common in lymphoma than in adenocarcinoma
MRI
- focal form: low signal intensity on T1-weighted images and intermediate signal intensity on T2-weighted images (slightly higher signal intensity than the pancreas but lower signal intensity than fluid), and shows faint contrast enhancement
- diffuse form: low signal intensity on T1- and T2-weighted MR images and shows homogeneous contrast enhancement, although small foci of reduced or absent enhancement are sometimes seen
Treatment and prognosis
Percutaneous or endoscopic core biopsy should be performed to establish the diagnosis .
Pancreatic lymphoma carries a better prognosis than adenocarcinoma because first-line treatment with chemotherapy is generally effective in producing long-term disease regression or remission. Surgery is not required in most cases.
Using complex treatment approaches, cure rates of up to 30% are reported for patients with primary pancreatic lymphoma. This prognosis is much better than the dismal 5% 5-year survival rate in patients with pancreatic adenocarcinoma .
Differential diagnosis
Imaging differential considerations include
For a diffuse bulkiness to the pancreas consider
Siehe auch:
- Akute Pankreatitis
- Pankreastumoren
- neuroendokrine Pankreastumoren
- Pankreasmetastasen
- solide Pankreastumoren
- Non-Hodgkin-Lymphom
- extranodal non-Hodgkin lymphoma
- multiple solid pancreatic tumors
- primäres Lymphom des Pankreas
und weiter:


 Assoziationen und Differentialdiagnosen zu Lymphombefall des Pankreas:
Assoziationen und Differentialdiagnosen zu Lymphombefall des Pankreas: