Pankreasmetastasen





Pancreatic metastases are uncommon and are only found in a minority (3-12%) of patients with widespread metastatic disease at autopsy. They account for only 2-5% of all pancreatic malignancies.
Epidemiology
Demographics will match those of the primary tumor, but in general, will be in elderly patients.
Clinical presentation
Most pancreatic metastases are asymptomatic and are found incidentally on imaging or at autopsy . If particularly large, especially if at the head of the pancreas, then local symptoms may include:
- jaundice: from CBD obstruction
- malabsorption: pancreatic insufficiency
- duodenal/gastric outlet obstruction
- gastrointestinal bleeding
Pathology
Although essentially any primary may eventually deposit in the pancreas, the most common primaries encountered include :
- renal cell carcinoma (RCC): one of the most common tumors that metastasize to the pancreas
- melanoma
- breast cancer
- lung cancer
- gastric cancer
- colorectal carcinoma (CRC)
- soft-tissue sarcoma
- prostatic cancer
- Merkel cell carcinoma (rare)
- hepatocellular carcinoma
- papillary thyroid carcinoma
- esophageal squamous cell carcinoma
- testicular seminoma
- rhabdomyoma
Radiographic features
Metastases to the pancreas do not have a predilection for any one part of the gland, and can have a variety of appearances :
- localized mass: 50-75%
- diffuse involvement: 5-45%
- multiple nodules: 5-15%
In general, they tend to be small lesions (0.5-2.0 cm) .
Ultrasound
Metastases appear as solid hypoechogenic masses located within the pancreatic parenchyma . Cysts are generally not a feature.
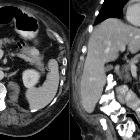
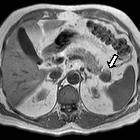
CT
Findings are non-specific, typically demonstrating a well-circumscribed mass which is iso- to hypodense relative to normal pancreas on non-contrast scans . Enhancement is usually present and heterogeneous but tends to be homogeneous in smaller lesions, and peripheral in larger lesions, presumably due to central necrosis . In general, the enhancement pattern resembles that of the primary tumor.
Calcification is rare (again depends on the primary).
Pancreatic ductal obstruction is common for head and body lesions, seen in up to ~40% of cases, and may be associated with CBD obstruction and intrahepatic biliary dilatation .
Treatment and prognosis
Treatment is targeted at local symptomatic control, with biliary stents or gastroenteric bypass for obstruction. In general, patients are treated with palliative intent, due to widespread metastatic disease.
Resection is usually not an option, except occasionally in the setting of solitary RCC metastasis .
Prognosis is universally poor, matching that of the metastatic primary.
Differential diagnosis
- pancreatic ductal adenocarcinoma
- pancreatic islet cell tumors: especially for vascular metastases, e.g. RCC
- autoimmune pancreatitis
- lymphoma
- splenule
Siehe auch:
- Pankreaskarzinom
- zystische Pankreasläsionen
- Autoimmunpankreatitis
- Hypervaskularisierte Pankreasläsionen
- neuroendokrine Pankreastumoren
- Lymphombefall des Pankreas
- intrapankreatische Nebenmilz
- solide Pankreastumoren
- Pankreasmetastasen (Nierenzellkarzinom)
- Pankreasmetastasen (Lungenkarzinom)
- Pankreasmetastasen (Schilddrüsenkarzinom)
- Pankreasmetastasen (Osteosarkom)
- Pankreasmetastasen (Rektumkarzinom)
- Pankreasmetastasen (Mammakarzinom)
und weiter:


 Assoziationen und Differentialdiagnosen zu Pankreasmetastasen:
Assoziationen und Differentialdiagnosen zu Pankreasmetastasen: