penetrating atherosclerotic ulcer










Penetrating atherosclerotic ulcers (PAU) are a pathology that involves the aortic wall. Along with aortic dissection and aortic intramural hematoma they can form the spectrum known as acute aortic syndrome.
Epidemiology
Typically, penetrating atherosclerotic ulcers are seen in older male patients with a history of hypertension (up to 92%), smoking (up to 77%) and coronary artery disease (up to 46%) as well as chronic obstructive pulmonary disease (24-68%) .
Penetrating atherosclerotic ulcers account for ~7.5% (range 2.3-11%) of all cases of acute aortic syndrome . In ~50% (range 42-61%) of cases, there are concurrent aortic aneurysms, most often in the abdomen .
Clinical presentation
Typically patients present with symptoms of an acute aortic syndrome, namely acute intense chest pain, often described as tearing, ripping, migrating or pulsating .
Some of the patients with penetrating atherosclerotic ulcers are asymptomatic and the diagnosis is made incidentally. In the previously cited article they cite the Mayo Clinic series in which just 75% of the patients had been symptomatic .
Pathology
The term "penetrating atherosclerotic ulcer" describes an ulcerating atherosclerotic lesion that penetrates the intima and progresses into the media. In the early stages, the lesions just ulcerate the intima and are often asymptomatic. With further progression, they ulcerate the media and lead to a hematoma of variable size within the media .
The penetrating atherosclerotic ulcer can resolve completely or stay stable, but they can also lead to aortic dissection, aortic saccular aneurysms and even spontaneous aortic rupture. There are conflicting reports about the most common course of penetrating atherosclerotic ulcers .
Location
There is a greater predilection to involve the mid to distal thoracic aorta .
Radiographic features
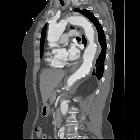
CT
On CT aortography, the typical finding is a contrast-filled, out-pouching of the wall of the aorta or into the thickened aortic wall in absence of an intimal flap or a false lumen. The protrusion is said to resemble a mushroom . These can progress to an intramural hematoma. Often there are signs of extensive atherosclerosis in other sites apart from the ulceration .
Usually, the ulcer is found in the descending part of the thoracic aorta. Ulcers of the aortic arch are less common, and rare in the ascending aorta .
Although associated pleural effusion correlates with clinical instability there are no validated imaging features for prediction of the course of a PAU . It is often difficult to determine if a PAU is the source of a patient's pain or if it is an incidental finding.
In follow-up studies increasing maximum diameter and depth of the ulcer is an obvious sign of progression . However, there is currently no consensus for ulcer depth or diameter that warrants treatment .
Transesophageal echocardiography
- usually, transesophageal echocardiography demonstrates a localized, crater-like protrusion of the aortic lumen into the thickened aortic wall
- often there are signs of extensive atherosclerosis in other sites apart from the ulceration
MRI and MRA
- T1-weighted SE sequences show a hyperintense hematoma in acute or subacute disease and can distinguish between hematoma and atherosclerotic plaque
- otherwise similar findings to CTA
DSA
- the typical finding is a contrast-filled, pouch-like protrusion of the aortic lumen
- mostly several oblique projections are required
Treatment and prognosis
No set guidelines on when to treat and practices vary between hospitals, however the general consensus is as follows:
- ascending aorta
- although the involvement of the ascending aorta in penetrating atherosclerotic ulcers is rare, the ulcers usually rupture
- therefore early/urgent or emergent surgical intervention is recommended
- descending aorta
- asymptomatic:
- may initially be managed with an aggressive (antihypertensive) medical therapy in combination with close clinical and radiographic follow-up
- annual CT imaging follow-up has been suggested
- may initially be managed with an aggressive (antihypertensive) medical therapy in combination with close clinical and radiographic follow-up
- symptomatic or signs of progression:
- higher risk for spinal cord ischemia
- endovascular stent-grafting (TEVAR)
- asymptomatic:
- iliac arteries
- generally asymptomatic/incidental and slow-growing
- mortality is determined by concurrent co-morbidities such as concurrent aortic aneurysm
Complications
Recognized complications include:
- transmural aortic rupture
- embolic phenomena
- pseudoaneurysm formation
- progressive aneurysmal dilatation
History and etymology
They were first described as a distinct clinical and pathological entity by Stanson et al. in 1986 .
Differential diagnosis
General imaging differential considerations include:
- focal indentation as part of irregularity along mural aortic plaque: could represent a non-penetrating atheromatous ulcer.
- aortic intramural hematoma
- aortic dissection
- saccular aneurysm
- (thoracic) aortic injury
Siehe auch:
- Pleuraerguss
- Aneurysma
- Aorta ascendens
- Chronisch obstruktive Lungenerkrankung
- Aortenbogen
- posttraumatisches Aneurysma spurium
- thorakale Aortendissektion
- Aortendissektion
- Aorta thoracica
- thorakale Aortenverletzungen
- mykotisches Aortenaneurysma
- inflammatorisches Aortenaneurysma
- intramurales Hämatom der Aorta
- Akutes Aortensyndrom
- PAU Klassifikation Aortenaneurysma
- endovascular stent-grafting
und weiter:


 Assoziationen und Differentialdiagnosen zu penetrierendes Aortenulkus (PAU):
Assoziationen und Differentialdiagnosen zu penetrierendes Aortenulkus (PAU):







