primary uveal malignant melanoma


















Malignant uveal melanomas, also referred to as choroidal melanomas, are the most common primary tumor of the adult eye .
Epidemiology
Malignant melanoma of the uvea is the most common primary intraocular malignancy and is predominantly seen in Caucasians . The incidence of these tumors increases with age, with only 2% of tumors found in patients younger than 20 years of age .
Clinical presentation
Clinical presentation depends on the location. When the tumor is located on the iris, then it may be apparent to the patient or friends and family as a brown nodule. Choroidal or ciliary body tumors are only identified incidentally on fundoscopy or as a result of retinal detachment or advanced disease.
Pathology
Uveal melanomas arise from the ciliary body or the choroid. Three histological types are recognized :
- mixed melanoma: containing both spindle B cell and epithelioid cells
- epithelioid melanoma
- necrotic melanoma
Radiographic features
Ultrasound
Ultrasound is an excellent modality for examining the globe and can visualize small plaque-like or discoid uveal melanoma, with a thickness of less than 3 mm, which are usually difficult to assess on CT or MRI. Features include :
- solid low to medium echotexture
- internal vascularity
- collar button shape
- this is the classic shape but not always the case
- represents tumor having broken through Bruch's membrane
- tumors may be irregular, lobulated or domed
Other features sometimes present include retinal detachment, posterior scleral bowing, choroidal excavation and vitreous or subretinal seeding. Additionally, larger tumors are often significantly sound attenuating .
CT
CT is able to identify most uveal melanomas which appear as elevated, hyperdense sharply marginated lenticular or mushroom-shaped lesions, which enhance with the administration of contrast.
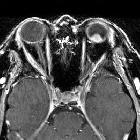
MRI
MRI is the modality of choice for assessment of malignant uveal melanomas :
- T1 or PD
- uveal melanomas are seen as moderately high signal mass lesion (melanin and hemorrhage are responsible for the high signal)
- associated exudative retinal detachment is moderately high signal
- T2
- moderately low signal mass lesion
- associated exudative retinal detachment is moderately high signal
- hemorrhagic subretinal fluid has a variable signal pattern
- T1 C+ (Gd)
- tumors enhance
- fat suppression useful in detecting extraocular extension
Treatment and prognosis
Treatment for uveal malignant melanoma depends on tumor size and clinician's preference. Options include photocoagulation, transpupillary thermotherapy (TTT), brachytherapy, hadrontherapy , local excision, or enucleation .
Poor prognostic factors for systemic disease include :
- older age: >60 years of age
- larger tumors
- anterior location within the globe
- epithelioid cells (i.e. mixed or epithelioid histology)
- extraocular extension, which usually occurs along the ciliary vessels and nerves, and less commonly along the optic nerve
Systemic metastases may be widespread (liver > lung > bone > kidney > brain> breast) . They can metastasize late to the liver, with delays of 10 to 15 year from the presentation.
Overall survival depends on tumor size, extraocular spread, and metastases. Even small (<10 mm diameter, <3 mm thickness) tumors still carry a 10-15% 5-year mortality .
Differential diagnosis
- retinoblastoma
- uveal metastases
- choroidal detachment
- choroidal hemangioma
- choroidal cyst
- uveal neurofibroma
- uveal schwannoma
See also
- ocular pathology
- ocular pathology (an approach)
Siehe auch:
- Uvea
- Retinoblastom
- Malignes Melanom
- Netzhautablösung
- Hirnmetastasen Malignes Melanom
- primary cutaneous melanoma
- melanoma of prostate
- Pathologien des Auges
- Aderhautablösung
- Aderhauthämangiom
- primäres malignes Melanom der Urethra
- Okulare Metastasen
- Retinale angiomatöse Proliferation
und weiter:


 Assoziationen und Differentialdiagnosen zu Aderhautmelanom:
Assoziationen und Differentialdiagnosen zu Aderhautmelanom:








