Metastasen in der Orbita








Orbital metastases are relatively uncommon, but some primary tumors do have a predilection to metastasize to the orbit.
This article concerns itself with extraocular metastases, rather than intraocular tumors or direct extension of tumors from neighboring regions. For a discussion of intraocular metastases please refer to uveal metastases.
Epidemiology
Extraocular orbital metastases are uncommon, accounting for 2-11% of all orbital neoplasms, and significantly less common than uveal metastases, which outnumber orbital metastases by 8 to 1 . The demographics of affected patients reflect the demographics of the primary tumors (see below).
Clinical presentation
In general, patients with metastatic disease do not develop orbital metastases, being identified clinically in <1% of cases. Prevalence is much higher in autopsy series, reflecting the high prevalence of asymptomatic orbital deposits .
In ~40% of patients who are symptomatic from orbital metastases (except for breast cancer metastases), orbital symptoms occur well before local symptoms from the primary tumor manifest, and as such is the first indication of advanced malignancy .
Unlike primary orbital tumors which most frequently present with proptosis and/or visual loss, orbital metastases most commonly present with diplopia . Pain is also frequently present.
Enophthalmos due to infiltration and desmoplasia is most frequently encountered with breast carcinoma metastases, although it may also be occasionally seen in metastases from gastrointestinal tract adenocarcinoma . This may be associated with hypoglobus.
Diagnosis is often known and widespread metastatic disease offers easier targets for biopsy. In cases where orbital metastases are isolated, a biopsy may be required to establish the diagnosis. This is usually performed as an open biopsy, to allow for adequate hemostasis .
Pathology
In adults, orbital metastases can be due to many different primaries
- breast cancer
- bronchogenic cancer
- prostate cancer
- gastrointestinal adenocarcinoma
- thyroid carcinoma
- renal cell carcinoma
- neuroblastoma
- Ewing sarcoma
- Wilms tumor
- leukemia
- pancreatic adenocarcinoma
- endometrial carcinoma
- ovarian carcinoma
- melanoma
- urothelial carcinoma of the urinary bladder
- non-Hodgkin lymphoma
- seminoma of testis
In children, the vast majority of orbital metastases are due to neuroblastoma .
Radiographic features
In contrast to uveal metastases which can be bilateral (up to 25%), extraocular orbital metastases are usually unilateral (with the exception of neuroblastoma) , and only infrequently primarily involve the extraocular muscles (with the exception of melanoma) , although secondary involvement as the metastasis grows is common . Thyroid and prostate metastases are frequently located in the bony margins of the orbit .
The superior lateral extraconal quadrant is most frequently involved although all parts of the orbit may be the site of metastatic deposit.
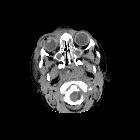
CT
CT appearances are variable. In most instances, soft tissue attenuating material is identified, located in the extraconal compartment . The morphology is variable, ranging from well-defined rounded lesions to diffusely infiltrating lesions .
In general, enhancement is present. Bony destruction may also sometimes be seen, and careful assessment of the remainder of the scan essential in identifying additional deposits.
MRI
MRI appearances are similar to CT, but the greater contrast resolution of MRI makes it invaluable in the assessment of orbital masses.
Fat-suppressed T2 and post-contrast T1 weighted images, with thin slice thickness and a reduced FOV is ideal and should include the cavernous sinuses.
- T1: isointense to muscle
- T2: hyperintense to muscle, hypointense to fat
- T1 C+ (Gd): enhancement present but variable
Treatment and prognosis
Treatment is primarily with radiotherapy, typically with a total dose of 30-40 Gy . Depending on the tumor histology chemotherapy may also be useful. Surgery is usually limited to patients with isolated orbital involvement without an identifiable (or a previously treated) primary.
Unfortunately, the discovery of orbital metastases usually indicates advanced and widespread metastatic disease and prognosis are dismal with the majority of patients succumbing to their illness within a year (average time from diagnosis to death is 4 months) .
Differential diagnoses
- primary orbital malignancy
- extraocular extension of an intraocular tumor
- tumors of the optic nerve
- orbital vascular lesion
- orbital infection
- thyroid-associated orbitopathy
- inflammatory/granulomatous conditions
Siehe auch:
- Sarkoidose
- Lungenkarzinom
- Nierenzellkarzinom
- intraorbitale Raumforderungen
- Aderhautmelanom
- Granulomatose mit Polyangiitis
- Neuroblastom
- inflammatorischer Pseudotumor der Orbita
- Ewing-Sarkom
- orbitales Lymphom
- Adenokarzinom der Prostata
- Schilddrüsenkarzinom
- Opticusgliom
- Orbitaphlegmone
- Meningeom Nervus opticus
- Nephroblastom
- Rhabdomyosarkom der Orbita
- Tumoren der Tränendrüse
- Orbita
- Neoplasien der Mamma
- Okulare Metastasen
- vaskuläre intraorbitale Läsionen
- thyroid associated obitopathy
und weiter:


 Assoziationen und Differentialdiagnosen zu Metastasen in der Orbita:
Assoziationen und Differentialdiagnosen zu Metastasen in der Orbita: