Orbita

The orbit is a feature of the face and contains the globe and its supporting structures, as well as many nerves and vessels.
Gross anatomy
In the adult, the orbit has a volume of approximately 30 mL, of which the globe occupies 6.5 mL. It has a roof, floor, medial and lateral wall. The orbit is open anteriorly where it is bound by the orbital septum, which forms part of the eyelids. Posteriorly, the orbit angles inward such that their apices communicate with the intracranial compartment via the optic canal and superior orbital fissure.
Contents
- globe
- extraocular muscles
- cranial nerves
- optic nerve (CN II)
- branches of the oculomotor nerve (CN III)
- superior division
- inferior division
- trochlear nerve (CN IV)
- branches of the ophthalmic division of the trigeminal nerve (CN Va)
- branches of the maxillary division of the trigeminal nerve (CN Vb)
- abducens nerve (CN VI)
- autonomic nerves and ganglia
- ciliary ganglion
- sympathetic root to the ciliary ganglion (parasympathetic root travels in the oculomotor nerve)
- arteries
- ophthalmic artery and its branches (ocular and orbital)
- infraorbital artery
- veins
- superior ophthalmic vein
- inferior ophthalmic vein
- infraorbital vein
- fat
- lacrimal gland
- fascia bulbi (Tenon's capsule)
Bony margins
The bony margins of the orbits, known as the bony orbit, are composed of seven bones:
- pars orbitalis of the frontal bone
- lacrimal bone
- lamina papyracea of the ethmoid bone
- orbital process of the zygomatic bone
- orbital surface of the maxillary bone
- orbital process of the palatine bone
- greater and lesser wings of the sphenoid bone
The four bones of the medial wall are remembered with this mnemonic.
Spaces
The orbit is divided by the musculofascial cone into 2 separate compartments:
Communications
The orbit communicates posteriorly with the intracranial cavity via the optic canal, through which the optic nerve and ophthalmic artery is transmitted. Immediately inferolateral to the optic canal is the superior orbital fissure, through which most neurovascular structures pass. The infratemporal fossa is accessed via the inferior orbital fissure, which is in direct continuation with the infraorbital foramen, through which the infraorbital nerve exits to supply the skin below the eye (and where it is often damaged by a blow-out fracture).
Medially, small communications with the paranasal sinuses are via the anterior ethmoidal foramen and posterior ethmoidal foramen.
Anteriorly, the supraorbital notch is closed inferiorly by the orbital septum forming a fibrous supraorbital foramen. The nasolacrimal duct drains the nasolacrimal sac via the nasolacrimal foramen.
Nerves of the orbit
There are many nerves within the orbit: see orbital nerve supply.
Stability of the globe
The fascial sheath of the eye (Tenon's fascia), orbital fat, obliques and bony attachment of the recti provide stability to the eyeball within the orbit and prevent it from sinking or retracting. See article titled 'stability of the eye'.
Downward displacement
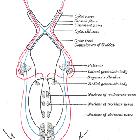
The fascial sheath of the eye (Tenon's fascia) prevents the eye from sinking. The fascia is applied like a bursa to the back of the eye, from the corneoscleral junction to the attachment of the optic nerve and is thickened over the extraocular muscles.
Over the lateral rectus, the tubular prolongation is thickened to form the lateral check ligament, which attaches to the marginal tubercle of Whitnall (bony elevation at the orbital surface of the zygoma). Over the medial rectus, this prolongation is thickened to form the medial check ligament, which attaches to the posterior lacrimal crest (of the lacrimal bone). Between these ligaments, the inferior part of the sheath is thickened to form the suspensory ligament of Lockwood, which supports the eye within the orbit.
The eye does not rest on the orbital floor but is held up (in fact, closer to the roof) by the suspensory ligament. As a result, the whole maxilla can be removed with the medial orbital wall up to the marginal tubercle without descent of the eye. Above this level removal of bone destroys the attachment of the suspensory ligament, hence the eye sinks down, and diplopia results.
Posterior displacement
The eyes always rotate about a fixed center, which is its own geometrical center. The contracting recti muscles do not displace the eye posteriorly due to:
See also
Siehe auch:
- Nervus trigeminus
- inflammatorischer Pseudotumor der Orbita
- Fissura orbitalis superior
- Orbitabodenfraktur
- Hirnnerven
- Nervus opticus
- Orbitaphlegmone
- Nervus abducens
- Nervus oculomotorius
- orbital pathology
- orbital spaces
- Nervus trochlearis
- Arteria ophthalmica
- äußere Augenmuskulatur
- Orbitafrakturen
und weiter:


 Assoziationen und Differentialdiagnosen zu Orbita:
Assoziationen und Differentialdiagnosen zu Orbita: