Orbitabodenfraktur

































Orbital blowout fractures occur when there is a fracture of one of the walls of orbit but the orbital rim remains intact. This is typically caused by a direct blow to the central orbit from a fist or ball.
Epidemiology
The blowout fracture is the most common type of orbital fracture and is usually the result of trauma. This is reflected in the demographics: it is more prevalent in young men. Female patients who present with clinical details that do not match the fracture such as 'falling' should raise concerns of intimate partner violence .
Clinical presentation
Orbital blowout fractures are usually the result of a direct blow to the orbit, which causes a sudden increase in intraorbital pressure. Decompression then occurs by fracture of one or more of the bounding walls of the orbit.
Although the causative trauma is usually substantial, presentation and diagnosis may be delayed in the setting of extensive soft tissue swelling and (by definition) an intact orbital rim. In particular, clinical findings of diplopia and restricted ocular motion may be temporarily masked by intraorbital swelling which can compensate for the traumatically-expanded osseous orbital volume .
Clinical findings associated with orbital blowout fracture may include:
- enophthalmos: due to increased orbital volume
- diplopia: due to extraocular muscle entrapment
- orbital emphysema: especially when the fracture is into an adjacent paranasal sinus (see: black eyebrow sign)
- malar region numbness: due to injury to the infraorbital nerve
- hypoglobus
Pathology
Different types of blowout fracture
Blowout fractures can occur through one or more of the orbital walls:
- inferior (floor)
- medial wall (lamina papyracea)
- superior (roof)
- lateral wall
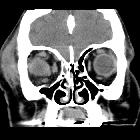
Inferior blowout fracture
Inferior blowout fractures are the most common. Orbital fat prolapses into the maxillary sinus and may be joined by prolapse of the inferior rectus muscle. In children, the fracture may spring back into place (see trapdoor fracture). Most fractures occur in the floor posterior and medial to the infraorbital groove .
In ~50% of cases, inferior blowout fractures are associated with fractures of the medial wall .
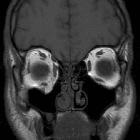
Medial blowout fracture
Medial blowout fractures are the second most common type, occurring through the lamina papyracea. Orbital fat and the medial rectus muscle may prolapse into the ethmoid air cells.
Superior blowout fracture
Pure superior blowout fractures (without associated orbital rim fracture) are uncommon. They are usually seen in patients with pneumatization of the orbital roof .
Fractures may only involve the sinus, the anterior cranial fossa (less common), or both sinus and anterior cranial fossa. Fractures communicating with the anterior cranial fossa are at risk for CSF leak and meningitis.
Lateral blowout fracture
Pure lateral blowout fractures are rare, as the bone is thick and bounded by muscle. If fractures are present they are usually associated with orbital rim or other significant craniofacial injuries.
Radiographic features
Plain radiograph
Radiographs are not recommended for the assessment of facial trauma due to poor sensitivity for injury.
However, if they are obtained, the diagnosis of fractures involving the inferior or medial wall may be suspected by visualization of fluid with the maxillary sinus and ethmoidal air cells, respectively . A few named signs have been described:
- orbital emphysema may result in a black eyebrow sign
- inferior herniation of the intraorbital fat may result in a "teardrop" sign
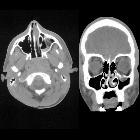
CT
CT is the modality of choice for assessment of the facial skeleton. A full assessment does not require the administration of contrast. Ideally, the acquisition should be performed using the thinnest detector settings, enabling thin-slice reconstructions along three orthogonal planes with a bone algorithm. Additional soft tissue algorithm reconstructions using larger slice thickness and 3D volumetric reconstruction are useful for assessing associated soft tissue injury and gauging facial asymmetry, respectively.
In addition to evaluating the location and extent of fracture(s), other features requiring assessment and reported include:
- presence of intraorbital (usually extraconal) hemorrhage: may result in stretching or compression of the optic nerve
- globe injury/rupture
- extraocular muscle entrapment: suspected if there is an acute change in angle of the muscle
- prolapse of orbital fat
Several imaging features are associated with late enophthalmos :
- surface area of fracture ≥2 cm
- ≥25-50% involvement of inferior or medial orbital walls
- collapse of internal orbital buttress or convex junctional bulge
- internal orbital buttress located at the union between medial and inferior orbital walls
- convex junctional bulge is the posterior continuation of the internal orbital buttress, supporting the orbital contents from posterior
- intraorbital soft tissue herniation volume ≥1.5 cm
- a linear relationship between the volume of intraorbital contents and depth of enophthalmos
Treatment and prognosis
Management of any globe injury generally takes precedence over fractures .
In general, there has been a trend toward conservative management of orbital blowout fractures. Initial post-traumatic diplopia or extraocular muscle impairment may improve over time, as edema or muscle injury resolves .
For orbital fractures without associated globe injury, immediate surgical management is reserved for cases where the risk of chronic impairment outweighs the risks of surgery. Although the modern transconjunctival incision technique has decreased eyelid complications associated with cutaneous eyelid approaches, surgery in the acute setting remains associated with risk of an iatrogenic eyelid, extraocular muscle, or optic nerve injury . This is in part because soft tissue swelling may require increased surgical exposure and retraction .
Potential indications for surgical repair include:
- significant enophthalmos
- significant diplopia
- muscle entrapment, especially with "trapdoor fracture" in children
- large area fractures
The timing of surgery is a subject of debate. Many surgeons elect for semi-delayed or late repair. This allows for assessment for noticeable enophthalmos, diplopia, or extraocular muscle impairment once the swelling has subsided . This must be balanced against the risk of developing fibrosis and more permanent structural impairment with longer delayed management .
Differential diagnosis
For old medial orbital blowout fractures consider:
Siehe auch:
- Meningitis
- Orbita
- black eyebrow sign
- trapdoor fracture
- spontaner Kollaps des Sinus maxillaris
- Emphysem der Orbita
- Orbitafrakturen
- Musculus rectus inferior
und weiter:


 Assoziationen und Differentialdiagnosen zu Orbitabodenfraktur:
Assoziationen und Differentialdiagnosen zu Orbitabodenfraktur: