wilms tumor
























Wilms tumor, also known as nephroblastoma, is a malignant pediatric renal tumor.
Epidemiology
Wilms tumors are the most common pediatric renal mass, accounting for over 85% of cases and accounts for 7% of all childhood cancers . It typically occurs in early childhood (1-11 years) with peak incidence between 3 and 4 years of age. Approximately 80% of these tumors are found before the age of 5 years. When part of a syndrome (see below) they occur even earlier, typically between 2 and 24 months of age .
There is no recognized gender predilection, however, presentation is a little later in females . The vast majority are unilateral with less than 5 % occurring bilaterally.
Clinical presentation
Clinical presentation is typically with a painless upper quadrant abdominal mass. Hematuria is seen in ~20% of cases and pain is uncommon. On examination hypertension due to excessive renin production is found in up to 25% of patients and acquired von Willebrand disease is seen in 8% .
Associations
Although most cases are sporadic and only 2% of cases are familial, a number of associations are recognized :
- overgrowth syndromes (WT2 gene)
- non-overgrowth syndromes (WT1 gene)
- WAGR syndrome
- Denys-Drash syndrome
- Frasier syndrome
- isolated abnormalities:
- cryptorchidism: 3%
- hemihypertrophy: 3%
- hypospadias: 2%
- sporadic aniridia
- renal fusion
Risk factors
Pathology
The tumor typically arises from mesodermal precursors of the renal parenchyma (metanephros). Increasingly gene loci are being implicated on chromosome 11 (WT1: 11p13 and WT2: 11p15) as well as WTX on chromosome X, B-catenin on chromosome 3 or TP53 on chromosome 17 .
On gross inspection, these tumors are usually well-circumscribed or macrolobulated. Hemorrhage and central necrosis are common findings .
Radiographic features
Wilms tumors are usually large heterogeneous solid masses which displace adjacent structures. Occasionally they may be mostly cystic.
Metastases are most commonly to lung (85%), liver and local lymph nodes . Similar to renal cell carcinoma tumor thrombus into the renal vein, IVC and right atrium is also characteristic of advanced disease. See also: Wilms tumor staging.
Plain radiograph
Abdominal x-ray typically reveals a large soft tissue opacity displacing bowel. This is only relevant if found incidentally since a radiograph should never be used for the assessment of an abdominal mass. The only exception would be a resource-poor setting where an abdominal radiograph is the only imaging modality available.
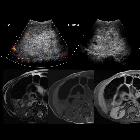
Ultrasound
Ultrasound is a very useful examination and in almost every situation will be the primary investigation of choice. It is helpful to localize the mass to the kidney and also distinguish from other causes of renal masses (e.g. hydronephrosis). Although many of the features seen on CT/MRI can also be identified on US, the former are required to adequately stage the disease and is established in protocols for Wilms tumor staging in North America and Europe .
Doppler examination can be performed to examine the renal vein and IVC to assess for the presence of tumor thrombus.
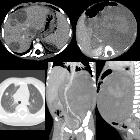
CT
Wilms tumors are heterogeneous soft-tissue density masses with infrequent areas of calcification (~15%) and fat-density regions. Enhancement is also patchy and allows for better delineation of the relationship between the mass and kidney. 10-20% of cases have lung metastases at the time of diagnosis .
MRI
Where MRI is available it is the investigation of choice for staging since it does not involve ionizing radiation. It is also the most accurate modality in assessing for IVC involvement where protocols have been optimized. These tumors appear heterogeneous on all sequences and frequently contain blood products.
- T1: hypointense
- T1 C+ (Gd): heterogeneous enhancement
- T2: hyperintense
Nuclear medicine
Bone scans are not routine as the tumor metastasizes to bones very late. F-18 FDG PET/CT is increasingly used as a problem-solving tool and to distinguish scar tissue from residual active tumor.
Treatment and prognosis
Unilateral Wilms tumors are, usually, treated by a combination of nephrectomy and chemotherapy. Occasionally chemotherapy can be administered prior to surgery to downstage the tumor . This is especially useful when tumors are bilateral.
Radiotherapy has a limited role, but may be employed in cases of peritoneal spread or incomplete resection .
Cure is now possible in ~90% of cases. Recurrence is seen both within the tumor bed, as well as distally within the lungs or liver .
History and etymology
This entity was popularized by Max Wilms in 1899, although prior descriptions had been published by Osler in 1880 and Birch-Hirschfeld in 1898 .
- Max Wilms (1867-1918), surgeon; Heidelberg, Germany
- Felix Victor Birch-Hirschfeld (1842-1899), physician; Leipzig, Germany
- William Osler (1849-1919), physician; Montreal, Canada
Differential diagnosis
General imaging differential considerations include:
- neuroblastoma: see neuroblastoma vs. Wilms tumor
- cystic partially differentiated nephroblastoma and pediatric cystic nephroma: appear identical to very cystic Wilms tumor
- clear cell sarcoma: generally indistinguishable on the bases of imaging, but may show early skeletal metastasis, a site which is unusual for Wilms tumor .
- renal rhabdoid tumor: generally, it can not be distinguished from Wilms on imaging, but the former has an established association with brain tumors, especially in the posterior fossa
- renal abscess
- angiomyolipoma
- childhood renal cell cancer: extremely rare in the pediatric population (outnumbered by Wilms tumors 30:1 ), it becomes more common in the second decade of life
See also
Siehe auch:
- Angiomyolipom
- Nierenzellkarzinom
- Neuroblastom
- Nierenabszess
- Nephroblastomatose
- pädiatrische Nierentumoren
- multilokuläres zystisches Nephrom
- paediatric cystic renal diseases
- Neuroblastom vs Nephroblastom
- Wilms-Tumor Metastasen
- recurrent Wilms tumour
und weiter:
- Angiomyolipom der Niere
- genitourinary curriculum
- Neurofibromatose Typ 1
- multizystische Nierendysplasie
- angeborene renale Anomalien
- Beckwith-Wiedemann-Syndrom
- Metastasen in der Orbita
- Nierentumor
- Metastasen im Hoden
- Pankreatoblastom
- claw sign
- Lungenmetastasen Wilmstumor
- small round blue cell tumours
- malignancies in childhood
- WAGR syndrome
- AML
- kongenitales mesoblastisches Nephrom
- Perlman-Syndrom
- fetale Tumoren
- metanephrisches Nierenadenom
- maligner rhabdoider Tumor
- Nephroblastom des Erwachsenen
- adult Wilm's Tumour in a pregnant lady
- maligner rhabdoider Tumor der Niere
- Denys-Drash syndrome
- wilms tumour staging
- wilms tumor and vasculitis
- Denys-Drash-Syndrom
- bilaterales Nephroblastom
- abdominal neuroblastoma
- Knochenmetastasen Nephroblastom
- Wilms' tumor with intracardiac extension
- multifocal Wilms tumor


 Assoziationen und Differentialdiagnosen zu Nephroblastom:
Assoziationen und Differentialdiagnosen zu Nephroblastom:




