multizystische Nierendysplasie
















Multicystic dysplastic kidney (MCDK) is a type of non-heritable pediatric cystic renal disease. It results in multiple cysts being formed in utero in the affected kidney.
Epidemiology
Unilateral incidence is estimated at 1:2500-4000. There may be a predisposition for the left kidney, a slightly higher incidence in males for unilateral MCDK and a higher incidence in females for bilateral MCDK.
Clinical presentation
MCDK develops in utero, and the diagnosis is often made either antenatally or in the early neonatal period if an ultrasound is performed. It may otherwise go unrecognised, and may be a common cause of renal agenesis, following complete involution during childhood.
Pathology
The affected kidney (or renal segment) has no functioning renal tissue and is replaced by multiple cysts. Two main types have been described :
- most common
- multiple small non-communicating renal cysts representing the dilated calyces
- atresia of the ureter and renal pelvis
- may sometimes regress spontaneously
- dominant cyst present in the renal pelvis
Genetics
The vast majority are sporadic and non-familial. Rarely autosomal dominant forms are seen .
Associations
Associated contralateral renal tract abnormalities are common (seen in ~50% of cases) and include:
- vesicoureteric reflux (VUR): most common and seen in up to 20%
- pelviureteric junction (PUJ) obstruction
- ureteral ectopia
- vesicoureteric junction (VUJ) obstruction
- ureterocoele
Syndromic associations include:
Radiographic features
The diagnosis of MCDK is often made antenatally with multiple small cysts becoming evident as early as the 15 week of gestation . Over time appearances may change dramatically, ranging from complete involution to large multicystic masses.
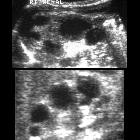
Ultrasound
Lobulated renal contour with multiple internal cysts of varying sizes and shapes: the renal parenchyma is usually fibrous and echogenic with absent or small hilar vessels. The cysts typically cluster and are non-communicating. Real time imaging is extremely useful to exclude any communication with the ureter and between each other.
MRI
The non-ionizing radiation imaging modality is an important consideration in the pediatric population. MCDK cysts are eloquently demonstrated on T2 sequences.
Nuclear medicine
MAG3 or DTPA scan: particularly useful in the hydronephrotic form to assess for associated obstructive uropathy. Although it may show some flow to the kidney and possible cortical uptake, generally a void is seen on the renal bed compared to the contralateral side, excretion is never seen.
Treatment and prognosis
A normal life expectancy can be expected as long as the contralateral kidney is normal. Bilateral MCDK is fatal. Controversy exists over the need for prophylactic surgical excision of an MCDK, justified on the grounds of a small risk of malignant transformation, more commonly in adults with a persistent MCDK (i.e. has not spontaneously resolved) . More recently, conservative management with follow-up has been recommended .
Complete spontaneous involution is said to occur in up to 60% of cases, but may take up to 10 years to occur . Longer term ongoing follow-up to assess what the lifetime rates of involution are in progress . If surgical resection is performed, it is done so early in life and is a simple and well-tolerated procedure .
Complications
Occasionally an MCDK may become infected or present with persistent mass effect or secondary hypertension .
Differential diagnosis
Given the variable appearance of MCDK's, some other entities need to be included in the differential including :
- hydronephrosis: fetal hydronephrosis: cystic spaces are interconnected
- cystic kidney diseases of childhood
- Wilms tumor
- tuberous sclerosis (TS)
- congenital mesoblastic nephroma: usually presents as solid lesions
- neonatal hydronephrosis
- autosomal dominant polycystic kidney disease
- pelviureteric junction obstruction
- parapelvic cyst
See also
Siehe auch:
- Tuberöse Sklerose
- Ureterozele
- Ureterabgangsstenose
- Meckel-Syndrom
- angeborene renale Anomalien
- einseitige Nierenagenesie
- fetal hydronephrosis
- Nephroblastom
- Zellweger-Syndrom
- kongenitales mesoblastisches Nephrom
- congenital cystic renal disease
- cystic renal disease
- cystic kidney diseases of childhood
- paediatric
und weiter:


 Assoziationen und Differentialdiagnosen zu multizystische Nierendysplasie:
Assoziationen und Differentialdiagnosen zu multizystische Nierendysplasie:






