Tuberöse Sklerose





















































Tuberous sclerosis, also known as tuberous sclerosis complex or Bourneville disease, is a neurocutaneous disorder (phakomatosis) characterized by the development of multiple benign tumors of the embryonic ectoderm (e.g. skin, eyes, and nervous system).
Epidemiology
Tuberous sclerosis has an incidence of 1:6000-12,000, with most being sporadic (see below) .
Clinical presentation
Tuberous sclerosis was classically described as presenting in childhood with a triad (Vogt triad) of:
The full triad is only seen in a minority of patients (~30%). Therefore, diagnostic criteria have been developed to aid the diagnosis of tuberous sclerosis.
See tuberous sclerosis diagnostic criteria .
When patients do not meet these criteria, they are sometimes referred to as manifesting a forme fruste of the condition.
Pathology
Spontaneous mutations account for 50-86% of cases , with the remainder inherited as an autosomal dominant condition. In the majority of such cases (80%) the mutation has been narrowed down to two tumor suppressor genes, both part of the mTOR pathway :
- TSC1: encoding hamartin, on chromosome 9q32-34
- TSC2: encoding tuberin, on chromosome 16p13.3 (accounts for most cases)
Radiographic features
Tuberous sclerosis has a significant number of manifestations, involving many organ systems. The most common radiographic manifestations are:
- cortical or subependymal tubers and white matter abnormalities
- renal angiomyolipomas
- cardiac rhabdomyoma(s)
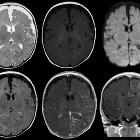
Neurological
- cortical/subcortical tubers: 50% are in the frontal lobe; high T2 and low T1 with only 10% of tubers showing enhancement; frequently calcify after two years of age
- subependymal hamartomas
- 88% are associated with calcification, although calcification absent in early childhood
- visible within the first six months of age
- variable signal, frequently high T1 and iso to high T2
- enhancement is variable and is not a useful feature in distinguishing them from subependymal giant cell astrocytomas (SGCA); only serial growth is reliable
- subependymal giant cell astrocytomas (SGCA)
- peak occurrence 8-18 years
- tend to be large and demonstrate growth
- tend to have intense enhancement
- white matter abnormalities
- variable appearance, with nodular, ill-defined, cystic and band-like lesions seen
- radial bands are thought to be relatively specific for TS
- retinal phakomas
- rarer findings
- cerebellar atrophy
- infarcts (due to occlusive vascular disorders)
- cerebral aneurysms
- dysgenesis of the corpus callosum
- Chiari malformations
- microcephaly
- arachnoid cysts
- chordoma
Abdominal
- renal angiomyolipoma(s)
- tuberous sclerosis accounts for 20% of all angiomyolipomas
- angiomyolipomas are seen in 55-75% of patient with tuberous sclerosis
- tend to be multiple, large and bilateral
- tend to grow and require surgical treatment, as the probability of hemorrhage is proportional to the size
- micro and macro aneurysms may be present
- fat may not be visible in up to 4.5%
- renal cysts: the TSC2 gene is located adjacent to the PCKD1 gene
- 18-53% of patients with tuberous sclerosis
- renal cell carcinoma and oncocytomas
- although rates of renal cell carcinoma are the same as in the general population, in patients with tuberous sclerosis, renal cell carcinoma tends to occur at a younger age
- retroperitoneal lymphangiomyomatosis (LAM)
- histologically identical to pulmonary LAM
- retroperitoneal cystic lesions
- chylous ascites, enlarged lymph nodes, dilatation of the thoracic duct
- gastrointestinal polyps
- pancreatic neuroendocrine tumors
- hepatic angiomyolipoma(s)
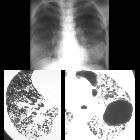
Thoracic
- lymphangioleiomyomatosis (LAM)
- rare (1%)
- some studies have described a lymphangiomyomatosis-like change to be present in 25-40% of female patients with tuberous sclerosis
- indistinguishable from sporadic LAM
- pneumothorax and chylous pleural effusions common
- ~80% 10-year survival
- multifocal micronodular pneumocyte hyperplasia (MMPH)
- rare
- characterized by multicentric well-demarcated nodular proliferation of type II pneumocytes
- benign, non-progressive
- differential diagnoses: miliary pulmonary opacities
- cardiac rhabdomyomas
- benign striated muscle tumor characterized by the presence of spider cells
- seen in 50-65% of patients with tuberous sclerosis
- 40-80% of patients with cardiac rhabdomyomas have tuberous sclerosis
- multiple or single
- typically involve the ventricular septum
- occur before the age of 1 year (75% of cases)
- typically regress before birth with spontaneous regression in 70% of children by age 4
- thoracic duct and aortic/pulmonary artery aneurysm
- myocardial fatty foci
Musculoskeletal
- sclerotic bone lesions: 40-66%
- hyperostosis of the inner table of the calvaria
- periosteal new bone
- scoliosis
- bone cysts
Skin
Cutaneous lesions are present in ~95% of cases, but are rarely appreciated radiographically :
- hypopigmented macules (ash leaf spots): seen in 90% of patients
- facial angiofibromas (Pringle nodules or adenoma sebaceum); seen in 75% of patients
- fibrous plaques of the forehead (15-20%)
- confetti lesions: variant of leukoderma spots
- shagreen patches: seen in 20-30% of patients
- periungual fibroma (Koenen tumors): 20% of patients
Treatment and prognosis
Treatment of seizures is essential and depending on the degree of intellectual disability, supportive care may be required. Treatment will be dictated by individual manifestations (e.g. subependymal giant cell astrocytomas, or retroperitoneal hemorrhage from renal angiomyolipoma).
Approximately 40% of patients die by age 35 from complications of one or more of the manifestations mentioned above .
History and etymology
Désiré-Magloire Bourneville (1840-1909) was a French neurologist that is notable by the initial description of tuberous sclerosis (“Bourneville disease”) in 1880.
John James Pringle (1855-1922) was a Scottish dermatologist that also studied this disease leading some books to refer to it as "Bourneville-Pringle disease”.
Heinrich Vogt (1875-1936) was a German neurologist that is notable by establishing the three pathognomonic clinical signs for tuberous sclerosis that became known as "Vogt triad”.
Siehe auch:
- Arachnoidalzyste
- Nierenzellkarzinom
- Angiomyolipom der Niere
- Chordom
- intraventrikuläre Neoplasien und Läsionen
- Skoliose
- Lymphangioleiomyomatose
- Mikrozephalie
- miliare Lungenherde
- intraventrikuläre Neoplasien und Läsionen - Überblick
- Dysgenesie des Corpus callosum
- Phakomatosen
- subependymales Riesenzellastrozytom
- Chiari-Malformation
- Rhabdomyom des Herzens
- multifocal micronodular pneumocyte hyperplasia (MMPH)
- Hirnarterienaneurysma
- subependymale Hamartome
- tuberous sclerosis diagnostic criteria
- skelettale Manifestationen bei tuberöser Sklerose
- angiomyolipomas (AML)
- subcortical hamartomas
- oncocytomas
und weiter:
- fetal intracranial calcification
- Bulbus-oculi-Verkalkungen
- Café-au-lait-Fleck
- multizystische Nierendysplasie
- multiple zystische Lungenherde
- diffuses intrinsisches Ponsgliom
- Chylothorax
- neuroradiologisches Curriculum
- Moyamoya-Erkrankung
- Makrozephalie
- intraventrikuläres Neurozytom
- Drusen der Papilla nervi optici
- Leukokorie
- retikuläres Muster
- Buschke-Ollendorff syndrome
- congenital hepatic fibrosis
- bilateral renal enlargement
- Milzhamartom
- Hemimegalencephalie
- bilateral megalencephaly
- Moyamoya-Muster
- hereditary renal cancer syndromes
- kortikale Malformation
- radial band sign
- Angiomyolipome der Niere bei tuberöser Sklerose
- bilateral giant renal angiomyolipomas
- Megaloenzephalie
- subkortikale Tubera
- perivascular epithelioid cell tumours
- renal cell carcinoma and multiple angiomyolipomas in a patient with tuberous sclerosis
- pulmonary lymphangioleiomyomatosis and renal angiomyolipoma
- fokale Fetteinlagerungen im Myokard
- giant cell astrocytoma in a patient with tuberous sclerosis
- renal cell carcinoma and tuberous sclerosis
- abdominal involvement in tuberous sclerosis complex
- tuberous sclerosis complex with lymphangiomyomatosis
- perivaskulärer epitheloidzelliger Tumor (PECom)
- tuberous sclerosis - involvement of the tibia
- tuberous sclerosis skeletal manifestations
- aneurysms in tuberous sclerosis
- Lymphangioleiomyom
- aortic aneurysms in tuberous sclerosis
- diffusion MRI in tuberous sclerosis
- radial bands sign
- Koenen-Tumor


 Assoziationen und Differentialdiagnosen zu Tuberöse Sklerose:
Assoziationen und Differentialdiagnosen zu Tuberöse Sklerose: