Rhombencephalosynapsis
















Rhombencephalosynapsis is a congenital abnormality of the cerebellum characterized by absence of the vermis and continuity of the cerebellar hemispheres, dentate nuclei, and superior cerebellar peduncles. It either occurs as an isolated anomaly (rare) or as part of wider cerebral malformation and it has variable degrees of neurological impairment.
Epidemiology
The condition is very rare and thought to be sporadic. No familial cases have been identified .
Clinical presentation
Clinical presentation includes truncal and/or limb ataxia, abnormal eye movements, head stereotypies, delayed motor development, and other features determined by supratentorial abnormalities (see below) . Overall patients tend to die in childhood or early adult life .
Associations
Rhombencephalosynapsis has been seen to be associated with:
- VACTERL
- Gomez-Lopez-Hernandez syndrome: comprises of rhombencephalosynapsis, developmental delay, scalp alopecia and trigeminal anesthesia
- vertebral fusion anomalies
Pathology
Embryologically rhombencephalosynapsis is now considered as a failure of vermian differentiation with the fused development of the cerebellar hemispheres, thought to result from an insult between the 28 and 44day of gestation . There is classically a transversely oriented single lobed cerebellum.
Rhombencephalosynapsis was traditionally thought to be a complete fusion of cerebellar hemispheres; however, off late cases of partial fusion have also been reported .
Radiographic features
MRI
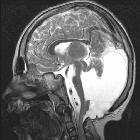
Rhombencephalosynapsis is best seen on MRI brain, and is characterized by :
- vermian abnormalities
- absent anterior (rostral) vermis
- deficient posterior (caudal) vermis
- nodulus tends to be formed
- fusion of the cerebellar hemispheres, with transversely oriented inferior cerebellar folia
- fusion of dentate nuclei
- fusion of the superior cerebellar peduncles
This usually results in an abnormally small posterior fossa, and an abnormally shaped fourth ventricle, which takes on a diamond (or key hole) shape .
Additional frequently associated abnormalities include:
- fusion of the thalami
- fusion of inferior colliculi
- absent septum pellucidum
- ventriculomegaly: often from aqueductal stenosis
- sutural synostosis
- other supratentorial abnormalities
- hypoplasia of the commissural system (corpus callosum, anterior commissure)
- hypoplasia of the anterior visual pathway
- agenesis of the posterior lobe of the pituitary
Treatment and prognosis
Variable clinical progression ranging from early death to varying degrees of cerebellar dysfunction and neurodevelopmental delay. Some patients may reach adulthood .
History and etymology
It was first reported by Heinrich Obersteiner (1847-1922), an Austrian neurologist, in 1914 .
Differential diagnosis
Imaging differential considerations include:
- Joubert syndrome
- Dandy-Walker spectrum
- Lhermitte-Duclos disease
- vermian hypoplasia
- tectocerebellar dysraphia
Siehe auch:
- Lhermitte-Duclos-Syndrom
- Gomez-Lopez-Hernandez syndrome
- Joubert-Syndrom
- Dandy Walker continuum
- fusionierte Thalami
- vermian agenesis
- fusion of the dentate nuclei
und weiter:


 Assoziationen und Differentialdiagnosen zu Rhombencephalosynapsis:
Assoziationen und Differentialdiagnosen zu Rhombencephalosynapsis: