superficial siderosis















Superficial siderosis is a rare condition which results from the deposition of hemosiderin along the leptomeninges, with eventual neurological dysfunction.
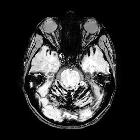
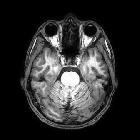
On imaging, it is classically characterized on MRI as a rim of low signal coating the surface of the brain or spinal cord, particularly noted with the gradient echo or susceptibility-weighted sequences.
Terminology
The literature is divided as to whether the term superficial siderosis should be confined to cases where there is no history of symptomatic subarachnoid hemorrhage, or whether it is a blanket term referring to the superficial deposition of hemosiderin, irrespective of cause.
For the purpose of this article, we take the latter definition.
Epidemiology
As there are many causes of recurrent or extensive subarachnoid hemorrhage, the demographics are ill-defined and represent those of the underlying cause. Cases have been reported in patients between 14 and 77 years of age . Overall, there is a male predilection (M:F 3:1) .
Clinical presentation
Symptoms can vary depending on the distribution of hemosiderin deposition. Typical symptoms include :
- sensorineural hearing loss
- most common, found in ~95% of patients
- bilateral and gradual
- cerebellar dysfunction (ataxia): ~90%
- pyramidal signs: ~75%
- other less common findings include
- dementia
- bladder incontinence
- other cranial nerve dysfunction
- sensory deficits
It is important to realize that the degree of imaging abnormality does not always correlate with the degree of clinical impairment .
Pathology
Superficial siderosis is thought to result from recurrent occult subarachnoid bleeds although the source of bleeding is not usually identified on imaging . Although it is common to see a small amount of hemosiderin deposition at the margins of a previous hemorrhage or surgical resection margin, a single episode of subarachnoid hemorrhage is usually not sufficient to result in this condition .
Vestibulocochlear nerve (CN VIII) dysfunction resulting in a sensorineural hearing loss is believed to be due to the combination of a long cisternal course (thus with ample exposure to the subarachnoid space) and the susceptibility of microglial cells (which have a role in myelination) to be damaged by iron compounds .
Etiology
A cause of recurrent subarachnoid hemorrhage is present in ~50% of cases :
- spinal dural defects
- traumatic cervical nerve root avulsion
- dural defect with spinal CSF collections/spinal cyst
- post-operative pseudomeningocoele
- intracranial neoplasms
- occult small ependymoma
- oligodendroglioma
- astrocytoma
- vascular abnormalities
- arteriovenous malformation (AVM)
- aneurysm
- fragile capillary regrowth after brain surgery
- cerebral amyloid angiopathy: seen in 60% of patients
- idiopathic: up to 46% of cases
Radiographic features
Angiography (DSA)
Usually unrewarding; will not demonstrate a point of bleeding .
MRI
MRI is the modality of choice for assessment and diagnosis of superficial siderosis. The findings are characteristic, with all pial and ependymal surfaces coated with low signal hemosiderin, particularly those of the brainstem and cerebellum (the cerebellar vermis and folia are excellent locations for identifying subtle deposits). In long-standing cases, cerebellar atrophy may also be present.
- T1: low signal
- T2: low signal
- GE (gradient echo): low signal with blooming
- SWI: low signal with blooming
As part of the workup for superficial siderosis, if no lesion is identified in the intracranial compartment, then imaging of the entire spinal canal should be performed (e.g. superficial hemosiderosis due to myxopapillary ependymoma) .
Treatment and prognosis
Unfortunately, no proven direct treatment exists for established siderosis, and workup is focused on identifying the causative lesion, although often even this is not possible. Iron chelating agents have been tried with limited anecdotal success .
When no correctable cause is identified, signs and symptoms are slowly progressive.
Siehe auch:
- Arteriovenöse Malformation
- Subarachnoidalblutung
- Aneurysma
- Oligodendrogliom
- Ependymom
- Pseudosubarachnoidalblutung
- Astrozytom
- spinales Ependymom des Filum terminale
- subpiale Blutung
- Hämosiderin
- Siderose der Leptomeningen
und weiter:


 Assoziationen und Differentialdiagnosen zu Superfizielle Hämosiderose der Leptomeningen:
Assoziationen und Differentialdiagnosen zu Superfizielle Hämosiderose der Leptomeningen:







