Leiomyosarkom des Pankreas
Irreversible
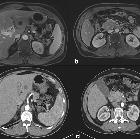
electroporation in a case of pancreatic leiomyosarcoma: a novel weapon versus a rare malignancy?. a MRI showing suspicious lesion in segment III of the liver prior to chemotherapy. b MRI showing pancreatic mass along with thrombosis of SMV prior to chemotherapy. c CT showing downsizing and minimal response of the segment III liver lesion after chemotherapy. d CT showing downsizing and minimal response of pancreatic mass after chemotherapy

Primary
leiomyosarcoma of the pancreas: report of a case treated by local excision and review of the literature. Pre-operative imaging. MRI scan: the dishomogeneous mass, arising from the pancreatic head (a). CT scan: no evidence of invasion of the surrounding tissues; CT venous phase: duodenal compression on the third duodenal part. (b) CT arterial phase: mass arising from the pancreatic head (c). 18F-FDG-PET-CT: moderate tracer uptake by the pancreatic lesion (d)
Leiomyosarkom des Pankreas
Pankreastumoren Radiopaedia • CC-by-nc-sa 3.0 • de
There are numerous primary pancreatic neoplasms, in part due to the mixed endocrine and exocrine components.
Classification
Classification based on function
- exocrine: ~99% of all primary pancreatic neoplasms
- pancreatic ductal adenocarcinoma ~90-95%
- cystic neoplasm
- intraductal papillary mucinous neoplasm (IPMN)
- endocrine: were previously referred to as islet cell tumors because they were thought to have originated from the islets of Langerhans, however, new evidence suggests that these tumors originate from pluripotential stem cells in ductal epithelium
- non-syndromic
- syndromic
- mesenchymal tumors
- although the great majority of both benign and malignant pancreatic neoplasms arise from pancreatic epithelial cells, mesenchymal tumors, while rare, can derive from the connective, lymphatic, vascular, and neuronal tissues of the pancreas
- they account for 1-2% of all pancreatic tumors and are classified according to their histologic origin
- other
Exocrine tumors
- ductal adenocarcinoma is by far the most common primary tumor, usually of the head (65%) and has a very poor prognosis.
- cystic neoplasms are further divided into (with some overlap):
- unilocular
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- macrocystic multilocular
- mucinous cystic neoplasm: usually body and tail
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- microcystic
- serous cystadenoma: usually head. 30% have a central scar
- cystic with a solid component
- macrocystic tumors can have solid component as well
- pancreatic adenocarcinoma may undergo cystic degeneration (8%)
- unilocular
- generally solid
See also: cystic pancreatic mass: differential diagnosis
Endocrine tumors
Endocrine tumors of the pancreas are divided into:
- functional: ~85%
- insulinoma: most common, 10% are malignant
- gastrinoma: second most common, 60% malignant
- glucagonoma: 80% malignant
- VIPoma: 75% malignant
- somatostatinoma: 75% malignant
- non-functional: ~15%
- third most common
- 85-100% malignant
- usually larger, as a result of lack of hormonal activity, the clinical presentations are usually delayed till they become large
Mesenchymal tumors
Account for 1-2% of all pancreatic tumors and are classified according to their histologic origin :
These are further discussed at pancreatic mesenchymal neoplasms
Classification based on location
Head
- ductal adenocarcinoma
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma
- pancreatoblastoma (rare and in children)
Body and tail
Intraductal
- intraductal papillary mucinous neoplasm (IPMN)
- pancreatic intraductal neoplasia (PanIN)
- intraductal tubular neoplasm (ITN)
- intraductal tubulopapillary neoplasm (ITPN)
- intraductal tubular adenoma (ITA)
- intraductal tubular carcinoma (ITC)
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Leiomyosarkom des Pankreas:
Assoziationen und Differentialdiagnosen zu Leiomyosarkom des Pankreas:

