Cystic lesions of the pancreas (differential)

Cystic
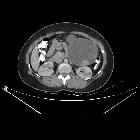
pancreatic lesions: MR imaging findings and management. Serous cystadenoma, “honeycomb” pattern. On contrast enhanced CT (a), a large hypodense lesion with tiny central enhancement can be appreciated in the body–tail of the pancreas. On T2w MRI, the lesion is hyperintense (b). On T1w dynamic imaging, the central enhancement is appreciable, especially with subtraction imaging (c), related to the enhancement of septa and stroma supporting the microcysts. MRCP (d)

Cystic
pancreatic lesions: MR imaging findings and management. Segmental MD-IPMN. At MRCP (a), a segmental dilatation of the MPD is appreciable in the body of the pancreas. The MPD upstream shows signs of chronic obstructive pancreatitis (finger-like dilatation of branch ducts), but the thickness of the pancreatic gland is normal (b). After 20 months, the dilatation of the MPD upstream is no longer appreciable (c), due to atrophy of the pancreatic gland (d)

Cystic
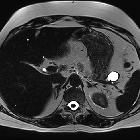
pancreatic lesions: MR imaging findings and management. Diffuse MD-IPMN. At MRCP (a), a diffuse enlargement of the MPD is appreciable through the gland with a grape-like dilatation of branch ducts (arrow) and without significant causes of obstruction nor calcifications both on T2w (b) and CT (c)

Cystic
pancreatic lesions: MR imaging findings and management. Microcystic serous cystadenoma with chronic obstructive pancreatitis. On T2w (a), a small lesion not clearly characterizable is appreciated in the neck of the pancreas. At MRCP (b), the wirsung duct is normal. c, d: Follow-up after 12 years: On T2w (c), the lesion is increased in size with a microcystic appearance and a large central scar, typical of a serous cystadenoma. At MRCP (e), a dilatation of wirsung duct with an appearance of chronic obstructive pancreatitis is clearly visible

Cystic
pancreatic lesions: MR imaging findings and management. Cystic complications of acute pancreatitis. a–d Pseudocyst. Patient with a previous interstitial edematous pancreatitis. At follow-up after 1 year, a cystic lesion with no septa or debris is appreciable in the tail of the pancreas, hyperintense on T2w (a), without high signal intensity on high b value DWI (b) and no enhancement after contrast media administration (c). At further follow-up after 6 months, the lesion is decreased in size (d). e–n: WON. A large necrotic collection is appreciable in a patient with necrotizing acute pancreatitis (e). After 1 year, a large collection with debris is still appreciable in the tail of the pancreas, clearly visible on T2w as cystic lesion with low signal intensity foci (f). Debris show inhomogeneous signal intensity on DWI (g), ADC map (h) and T1 unenhanced (i), but do not show any enhancement after contrast media administration (l, m). On T2 HASTE coronal view, the caudal extension of the collection is appreciable (n)

Cystic
lesions of the pancreas (differential) • Abdominal splenosis - Ganzer Fall bei Radiopaedia
Cystic
lesions of the pancreas (differential) • Pancreatic hydatid cyst - Ganzer Fall bei Radiopaedia

Cystic
lesions of the pancreas (differential) • Von Hippel-Lindau disease - pancreatic manifestations - Ganzer Fall bei Radiopaedia

Cystic
lesions of the pancreas (differential) • Solid pseudopapillary tumor of the pancreas - Ganzer Fall bei Radiopaedia

Cystic
lesions of the pancreas (differential) • Pancreatic mucinous cystadenoma - Ganzer Fall bei Radiopaedia

Cystic
lesions of the pancreas (differential) • Solid pseudopapillary tumor of the pancreas - Ganzer Fall bei Radiopaedia

Cystic
lesions of the pancreas (differential) • Pancreatic pseudocysts - Ganzer Fall bei Radiopaedia

Cystic
pancreatic lesions: MR imaging findings and management. Multifocal BD-IPMN. At MRCP in coronal (a) and axial (b) projection, several round dilatations of branch ducts in thigh connection with the MPD can be appreciable

Cystic
pancreatic lesions: MR imaging findings and management. Von Hippel–Lindau. Several cysts are visible on T2w: multifocal SCN

Cystic
pancreatic lesions: MR imaging findings and management. Serous cystadenoma, pseudosolid pattern. A small hypervascular lesion in the body of the pancreas is visible at contrast-enhanced CT, arterial phase (a). On T2w, the lesion is hyperintense (b), with no high signal intensity at DWI b 800 (c). At MRCP (d), the cystic components are well recognizable (arrow) and MPD is normal. e–h Follow-up at 5 years. A slight increase in size can be appreciable with no others significant changes. At ADC map (g), the lesion is clearly hyperintense due to cystic content

Cystic
pancreatic lesions: MR imaging findings and management. Serous cystadenoma, macrocystic pattern. Female, 57 yo. A large cist with thick walls is visible in the body of the pancreas with no nodules or enhancing septa both on T2w (a) and T1w before (b) and after contrast media administration (c) with atrophy of the tail (arrow in b). At MRCP (d), a dilatation of the MPD upstream is recognizable (arrow). Due to the high suspicious of a mucinous cystadenoma, the lesion was resected, and at pathology, a serous cystoadenoma was diagnosed

Cystic
pancreatic lesions: MR imaging findings and management. Acinar cell cystadenoma. At MRCP (a), there are several small cysts thought the pancreas. On T2w (b), some small hypointense foci are appreciable in the tail of the pancreas which at CT show up to be calcifications (c). At biopsy, an acinar cell cystoadenoma was found

Cystic
pancreatic lesions: MR imaging findings and management. Mucinous cystadenoma, multilocular pattern. On T2w axial sequence (a), a large multilocular cyst is appreciable in the tail of the pancreas. The multilocular pattern is better appreciable on coronal T2w sequence (b). Administration of paramagnetic contrast media was avoided as patient was pregnant. On axial T1w scan (c), an hyperintense deposit is appreciable in the lower part of the cyst, corresponding to mucin deposit

Cystic
pancreatic lesions: MR imaging findings and management. Mucinous cystadenoma, multilocular pattern. At unenhanced CT (a), a large cyst with a tiny septum is visible in the tail of the pancreas, which shows a slight enhancement after contrast media administration (b). On T1w fat-saturated GRE image (c), some hyperintense foci are visible in the inferolateral aspect of the cyst, which do not show significant enhancement after injection of paramagnetic contrast media (d), related to mucin content

Cystic
pancreatic lesions: MR imaging findings and management. Retention cyst. A small cyst is observed on T2w (a) and MRCP (b), without evidence of a mass. On a follow-up study two years later, a focal obstruction of the main pancreatic duct appeared with chronic obstructive pancreatitis features upstream (c, d), all findings of high suspicion of malignancy (pancreatic carcinoma on histology). (From: Morana G, Faccinetto A, Venturini S: Pancreas. In: Vanzulli A, Colagrande S, Grazioli L, Morana G (eds), MRI of the abdomen—technique and imaging findings. Poletto, Milan, 2021)

Cystic
pancreatic lesions: MR imaging findings and management. Solid pseudopapillary neoplasm. On T2w (a), a large cystic lesion with solid components is appreciable in the tail of the pancreas. The solid component shows high signal on DWI b 800 (b) and restricted diffusion at ADC map (c) and contrast enhancement on T1w after paramagnetic contrast media administration (d–f)

Cystic
pancreatic lesions: MR imaging findings and management. Cystic PNET. On T2w (a), a small hyperintense lesion with tiny septa is appreciable in the body of the pancreas. At T1w (b), during injection of paramagnetic contrast media an intense rim enhancement can be appreciable in the arterial phase (arrow). On DWI (c), no restricted diffusion can be appreciated and the lesion appears hyperintense at ADC map (d). After surgical removal, a G1 PNET was diagnosed at pathology

Cystic
pancreatic lesions: MR imaging findings and management. Chronic obstructive pancreatitis. At MRCP (a), a diffuse dilatation of the main pancreatic duct is appreciable through the gland with finger-like dilatation of branch ducts (arrow). At T2w, a defect in the prepapillary portion of the wirsung duct is appreciable (arrow). At unenhanced CT (c), a gross calcification is visible in the head of the pancreas, related to the intraductal calculus, responsible for the dilatation of the wirsung duct upstream, not visible on axial T2w (d)

Cystic
pancreatic lesions: MR imaging findings and management. Evolution of a mixed MD-IPMN. At T2w (a) and MRCP (b), a dilatation of a branch duct in the tail of the pancreas with a slight enlargement of the MPD in the tail. After 5 years, a diffuse dilatation of the MPD is appreciable

Cystic
pancreatic lesions: MR imaging findings and management. Unifocal BD-IPMN. On T2w (a) and MRCP (b), a cystic lesion with tiny septa is appreciable in the head of the pancreas. At T1w after paramagnetic contrast media injection (c), the septa show a slight enhancement. At DWI b 800 (d), no restriction diffusion can be observed
Cystic
lesions of the pancreas (differential) • Pancreatic neuroendocrine tumor - cystic - Ganzer Fall bei Radiopaedia
The differential for cystic lesions of the pancreas includes:
- unilocular
- pancreatic pseudocyst
- intraductal papillary mucinous neoplasm (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- simple pancreatic cyst
- pancreatic cysts occur in association with
- macrocystic: multilocular
- mucinous cystic neoplasm of pancreas: usually body and tail
- intraductal papillary mucinous neoplasm (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- acinar cell cystadenocarcinoma
- hydatid cyst
- microcystic
- serous cystadenoma: usually head; 30% have a central scar
- cystic with a solid component
- walled-off pancreatic necrosis
- macrocystic tumors can also have a solid component
- solid pseudopapillary tumor of pancreas
- primary ductal pancreatic tumor with cystic degeneration
- cystic degeneration of islet cell tumors (neuroendocrine tumors)
- cystic teratoma
- metastases to pancreas
Retroperitoneal lesions (extrinsic to the pancreas) can mimic pancreatic cystic lesions, when close to the gland. Examples include:
- cystic lymphadenopathy (e.g. necrotic)
- duodenal diverticulum
Practical points
The American College of Radiology (ACR) published guidelines on managing incidental cystic pancreatic lesions in 2017.
Siehe auch:
- Duodenaldivertikel
- Pankreaspseudozyste
- zystische Fibrose
- Insulinom
- intraduktale papillär muzinöse Neoplasie
- autosomal-dominante polyzystische Nierenerkrankung
- seröses Zystadenom des Pankreas
- muzinöses Zystadenom des Pankreas
- Morbus Hippel-Lindau
- solider pseudopapillärer Tumor des Pankreas
- Pankreasmetastasen
- Hamartom des Pankreas
- muzinös zystische Neoplasien des Pankreas
- seröses Zystadenokarzinom Pankreas
- serös zystische Neoplasie des Pankreas
- zystischer neuroendokriner Tumor des Pankreas
- Azinuszell-Zystadenom des Pankreas
- Retentionszyste Pankreas
- lymphoepitheliale Zyste des Pankreas
- ductal pancreatic tumour
- acinar cell cystadenocarcinoma
und weiter:
- Pankreaskarzinom
- Choledochuszyste
- Pankreastumoren
- Choledochozele
- solide Pankreastumoren
- Pankreaszyste
- chronische kalzifizierende Pankreatitis
- muzinöses Zystadenokarzinom des Pankreas
- pancreatic cystadenoma
- Dermoidzyste des Pankreas
- mucinous cystadenocarcinoma of pancreas with cystic liver metastases
- multiple zystische Pankreasläsionen
- chronisch obstruktierende Pankreatitis
- mikrozystisches seröres Zystadenom des Pankreas
- Lymphangiom des Pankreas
- Pankreasabszess


 Assoziationen und Differentialdiagnosen zu zystische Pankreasläsionen:
Assoziationen und Differentialdiagnosen zu zystische Pankreasläsionen:








