seltene Pankreastumoren

Imaging
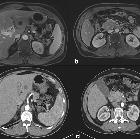
findings for pancreatic Hamartoma: two case reports and a review of the literature. The lesion showed a hypoechoic mass in the pancreatic head on US (a). Axial CT of the abdomen (plain scan and venous phase) showing a 2.9-cm iso-density lesion in the pancreatic head that was well-defined after enhancement (b-c). Axial pancreatic MRI showing a solid lesion with several small cystic lesions, T1WI showed hypointensity (d), T2WI showed iso- to high-intensity (e), and DWI showed iso-intensity (F); the lesion had obvious progressive enhancement (g-i)

Extra-gastrointestinal
stromal tumor of the pancreas: case report and review of the literature. Abdominal CT scan showing a 2-cm, contrast-enhanced mass (arrow) in the uncinate process of the pancreas.

Osteoclast–type
giant cell tumour of the pancreas: a case report. Ultrasound showed a solid heterogeneus mass (yellow arrow), apparently in the pancreas head, with associated Wirsung dilatation (green arrow).
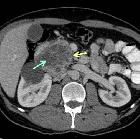
Osteoclast–type
giant cell tumour of the pancreas: a case report. Axial CT showed a heterogeneous mass (yellow arrow), with contrast enhancement in solid areas and necrotic component within the tumour (green arrow).

Perivascular
epithelial cell tumor (PEComa) of the pancreas: a case report and review of previous literatures. Imaging studies. a Ultrasonography showed that gourd-shaped hypo- and iso-echoic mass, 56 mm in size, was detected in the pancreatic head and body. b Enhanced computer tomography showed that solid well-circumscribed low-density mass, 7 cm in diameter, was located in the pancreatic head and body. c Heterogeneously enhanced mass was detected in the pancreatic body by gadolinium-enhanced MRI. d Endoscopic retrograde pancreatography (ERP) showed that main pancreatic duct was slightly deviated downward because of locoregional pressure effect, but direct invasion to the main pancreatic duct was not evident

Imaging
findings for pancreatic Hamartoma: two case reports and a review of the literature. The lesion showed a hypoechoic mass in the pancreatic head on US (a). Axial CT of the abdomen (plain scan and venous phase) showing a 1.4-cm iso-density lesion in the pancreatic head that was well-defined after enhancement (b-c). Axial pancreatic MRI showing a solid lesion, T1WI showed hypointensity (d), T2WI showed iso-intensity (e), DWI showed iso-intensity (f), the lesion had obvious progressive enhancement (g-i)

Primary
pancreatic glomus tumor invading into the superior mesenteric vein: a case report. Dynamic-CT scan (a early arterial phase, b late arterial phase, c and d portal phase). Dynamic-CT scan revealing a hypovascularized tumor (yellow arrowhead) invading the superior mesenteric vein (blue arrowhead)

A rare case
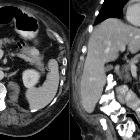
report of pancreatic low-grade fibromyxoid sarcoma (LGFMS). CT scan abdomen/pelvis with and without contrast. Axial (A, B) and coronal (C, D) views demonstrating pancreatic mass
Irreversible
electroporation in a case of pancreatic leiomyosarcoma: a novel weapon versus a rare malignancy?. a MRI showing suspicious lesion in segment III of the liver prior to chemotherapy. b MRI showing pancreatic mass along with thrombosis of SMV prior to chemotherapy. c CT showing downsizing and minimal response of the segment III liver lesion after chemotherapy. d CT showing downsizing and minimal response of pancreatic mass after chemotherapy

Pancreatic
acinar cell carcinoma with extension into the main pancreatic duct: a case report. a Multi-detector row computed tomography (MDCT) shows a slightly enhanced round tumor and the dilated caudal main pancreatic duct (MPD). b Magnetic resonance cholangiopancreatography (MRCP) demonstrates mild dilatation of cranial MPD and severe dilatation of caudal MPD. Cystic lesion [suspicious intraductal papillary mucinous neoplasm (IPMN)] is visible in the neck of the pancreas. c MDCT shows a tumor with downstream progression until the left side of IPMN. d A coronal view shows intraductal tumor mass extends to the left side of the IPMN
seltene Pankreastumoren
Pankreastumoren Radiopaedia • CC-by-nc-sa 3.0 • de
There are numerous primary pancreatic neoplasms, in part due to the mixed endocrine and exocrine components.
Classification
Classification based on function
- exocrine: ~99% of all primary pancreatic neoplasms
- pancreatic ductal adenocarcinoma ~90-95%
- cystic neoplasm
- intraductal papillary mucinous neoplasm (IPMN)
- endocrine: were previously referred to as islet cell tumors because they were thought to have originated from the islets of Langerhans, however, new evidence suggests that these tumors originate from pluripotential stem cells in ductal epithelium
- non-syndromic
- syndromic
- mesenchymal tumors
- although the great majority of both benign and malignant pancreatic neoplasms arise from pancreatic epithelial cells, mesenchymal tumors, while rare, can derive from the connective, lymphatic, vascular, and neuronal tissues of the pancreas
- they account for 1-2% of all pancreatic tumors and are classified according to their histologic origin
- other
Exocrine tumors
- ductal adenocarcinoma is by far the most common primary tumor, usually of the head (65%) and has a very poor prognosis.
- cystic neoplasms are further divided into (with some overlap):
- unilocular
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- macrocystic multilocular
- mucinous cystic neoplasm: usually body and tail
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma uncommonly uni/macrolocular
- microcystic
- serous cystadenoma: usually head. 30% have a central scar
- cystic with a solid component
- macrocystic tumors can have solid component as well
- pancreatic adenocarcinoma may undergo cystic degeneration (8%)
- unilocular
- generally solid
See also: cystic pancreatic mass: differential diagnosis
Endocrine tumors
Endocrine tumors of the pancreas are divided into:
- functional: ~85%
- insulinoma: most common, 10% are malignant
- gastrinoma: second most common, 60% malignant
- glucagonoma: 80% malignant
- VIPoma: 75% malignant
- somatostatinoma: 75% malignant
- non-functional: ~15%
- third most common
- 85-100% malignant
- usually larger, as a result of lack of hormonal activity, the clinical presentations are usually delayed till they become large
Mesenchymal tumors
Account for 1-2% of all pancreatic tumors and are classified according to their histologic origin :
These are further discussed at pancreatic mesenchymal neoplasms
Classification based on location
Head
- ductal adenocarcinoma
- intraductal papillary mucinous neoplasms (IPMN)
- serous cystadenoma
- pancreatoblastoma (rare and in children)
Body and tail
Intraductal
- intraductal papillary mucinous neoplasm (IPMN)
- pancreatic intraductal neoplasia (PanIN)
- intraductal tubular neoplasm (ITN)
- intraductal tubulopapillary neoplasm (ITPN)
- intraductal tubular adenoma (ITA)
- intraductal tubular carcinoma (ITC)
Siehe auch:
- Pankreaslipom
- Pankreastumoren
- Azinuszellkarzinom des Pankreas
- neuroendokrine Pankreastumoren
- Hamartom des Pankreas
- benigne Pankreastumoren
- Riesenzelltumor des Pankreas
- kindliche Pankreastumoren
- Lymphangiom des Pankreas
- Angiomyolipom des Pankreas
- mesenchymale Pankreastumoren
- Leiomyosarkom des Pankreas
- perivaskulärer epitheloidzelliger Tumor (PECom) des Pankreas
- Gastrointestinaler Stromatumor des Pankreas
- Neurofibrom des Pankreas
- Plattenepithelkarzinom des Pankreas


 Assoziationen und Differentialdiagnosen zu seltene Pankreastumoren:
Assoziationen und Differentialdiagnosen zu seltene Pankreastumoren:


perivaskulärer
epitheloidzelliger Tumor (PECom) des Pankreas