Plantarfasziitis



















Plantar fasciitis refers to inflammation of the plantar fascia of the foot. It is considered the most common cause of heel pain.
Clinical presentation
Pain on the undersurface of the heel on weight-bearing is the principal complaint. It can be worse when weight is borne after a period of rest (e.g. in the morning) and eases with walking. Passive dorsiflexion of the toes may exacerbate discomfort.
Pathology
It is generally a low-grade inflammatory process involving the plantar aponeurosis with or without the involvement of the perifascial structures.
It can arise from several factors:
- mechanical: stress of repetitive trauma (more common)
- degenerative
- systemic: as an enthesopathy in association with seronegative spondyloarthropathies
Radiographic features
Plain radiograph
Plain film features are non-specific but may show an associated plantar calcaneal spur although this is also seen in asymptomatic individuals. The thickness of the fascia can be increased to more than 4.5 mm.
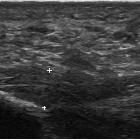
Ultrasound
Often the initial imaging modality of choice. Ultrasound typically shows increased thickness of the fascia (>4.5 mm) and a hypoechoic fascia .
MRI
Signal characteristics of affected tissues include:
- T1/PD: intermediate signal
- T2: high signal
- STIR: very sensitive in the detection of both fascial and perifascial edema, which appear as poorly marginated areas of high signal intensity
Other MRI features include:
- plantar fascial thickening: often fusiform and typically involves the proximal portion and extends to the calcaneal insertion
- increased T2/STIR signal intensity of the proximal plantar fascia
- edema of the adjacent fat pad and underlying soft tissues
- limited marrow edema within the medial calcaneal tuberosity may also be seen
Treatment and prognosis
Management options are usually conservative. Local injection of steroids +/- local anesthetic may be useful to manage symptoms. Ultrasound-guided steroid injection has been shown to be effective in short-term (four-week) pain relief with reduced thickness of the plantar fascia at three months . A posterior tibial nerve block can be performed prior for a less painful plantar fascia injection.
Specific plantar fascia stretching exercises performed daily have been shown to reduce short-term (8 weeks) and long-term (2 years) pain .
Other supportive measures include weight reduction in obese patients, rest, non-steroidal anti-inflammatory drugs (NSAIDs) and reduction of weight-bearing pressure (soft rubber heel pad, molded orthosis, or heel cup or soft-soled shoes).
See also
Siehe auch:
- Morbus Bechterew
- Psoriasisarthritis
- Morbus Ledderhose
- plantarer Fersensporn
- Plantaraponeurose
- Plantarvenenthrombose
- Fasziitis
und weiter:


 Assoziationen und Differentialdiagnosen zu Plantarfasziitis:
Assoziationen und Differentialdiagnosen zu Plantarfasziitis:



