psoriatic arthritis





























Psoriatic arthritis (PsA) is an inflammatory arthritis associated with psoriasis. It is usually negative for rheumatoid factor and hence classified as one of the seronegative spondyloarthritides.
Epidemiology
Overall prevalence is ~0.5% (range 0.1-1%), however, it affects up to ~25% (range 6-41%) of patients with psoriasis . In contrast to many other arthropathies, there is no gender predilection in psoriatic arthritis. The median age of diagnosis is 48 years .
Clinical presentation
Dermatological features of psoriasis precede arthritis in ~65% (range 60-70%) whereas arthritic symptoms proceed dermatological features in 15-20% . There is a strong association with nail involvement, particularly for distal interphalangeal joint arthritis. It most commonly presents as an asymmetrical oligo-arthritis with spondylitis common; oligo-arthritis may progress to polyarthritis in the clinical course of the disease .
Pathology
Both environmental and genetic factors are thought to play a role. Up to 60% are HLA-B27 positive . A proportion of patients have serum rheumatoid factor .
Extra-articular manifestations are common :
- ocular: uveitis, conjunctivitis
- gastrointestinal: inflammatory bowel disease
- cardiac: rhythm disturbances (e.g. bundle branch block)
- urogenital: urethritis, prostatitis, balanitis, cervicitis, vaginitis
Classification
One of the classification systems is the one by Moll and Wright, which classifies PsA into five subtypes:
Associations
PsA is associated with :
- obesity
- hypertension
- insulin resistance / type 2 diabetes
- hyperlipidemia
Radiographic features
The hallmark of PsA is the combination of erosive change with bone proliferation, in a predominantly distal distribution (e.g. interphalangeal more than metacarpophalangeal joints). The disease most commonly involves the hands, followed by feet. It can also affect sacroiliac joints and spine. Knees, elbows, ankles, and shoulders are less frequently involved .
In the hands and feet, the pattern of distribution may be that of a symmetric polyarthropathy, or asymmetric oligoarthropathy, with a distal predominance.
Imaging findings include:
- enthesitis and marginal bone erosions; "pencil-in-cup" deformities are common, but not pathognomonic for PsA
- bone proliferation results in an irregular, “fuzzy” appearance to the bone around the affected joint
- joint subluxation or interphalangeal ankylosis may be present
- periostitis: may appear as a periosteal layer of new bone, or as irregular thickening of the cortex itself
- dactylitis: which can present as a “sausage digit” which refers to soft tissue swelling of a whole digit; ultrasound examination of a sausage digit demonstrates underlying synovitis and tenosynovitis
- acro-osteolysis
- arthritis mutilans: osteolysis and articular collapse can cause a phenomenon referred to as "telescoping fingers"
- ivory phalanx: classically involving the distal phalanx of the great toe
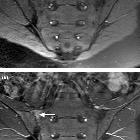
- sacroiliitis: often asymmetrical
- spondylitis: asymmetric paravertebral ossifications and relative sparing of the facet joints
Differential diagnosis
General imaging differential considerations include:
- rheumatoid arthritis
- there is an MCP joint predominance in rheumatoid arthritis (RA) vs interphalangeal predominant distribution in PsA
- bone proliferation not a feature in RA
- osteoporosis not a feature in PsA
- erosive osteoarthritis
- “gull-wing” central erosions are present in erosive OA vs “mouse ears” peripheral bare area erosions in PsA
- reactive arthritis (Reiter syndrome)
- tends to involve feet > hands
Siehe auch:
und weiter:
- Parasyndesmophyten
- Sakroiliitis
- Pencil-in-cup deformity
- Akroosteolyse
- Pencil-in-cup-Zeichen
- radiologisches muskuloskelettales Curriculum
- Jaccoud-Arthropathie
- Fersensporn
- sausage digit
- conditions involving skin and bone
- plantarer Fersensporn
- Plantarfasziitis
- Rheuma Differentialdiagnose
- musculoskeletal manifestations of AIDS
- temporomandibular joint inflammation
- vertebral body squaring
- spondyloarthropathy
- Befallsmuster Arthritis
- palindromer Rheumatismus
- seronegative Spondyloarthropathie
- Psoriasisarthritis ISG
- haemochromatosis - skeletal manifestations
- muskuloskelettale Manifestationen Hämochromatose
- licked candy stick appearance
- muskuloskelettale Manifestationen rheumatoide Arthritis


 Assoziationen und Differentialdiagnosen zu Psoriasisarthritis:
Assoziationen und Differentialdiagnosen zu Psoriasisarthritis:



