Arteria-mesenterica-superior-Syndrom





























Superior mesenteric artery (SMA) syndrome, also known as Wilkie syndrome or cast syndrome or aortomesentric duodenal compression syndrome, is a rare acquired vascular compression disorder in which acute angulation of the superior mesenteric artery (SMA) results in compression of the third part of the duodenum, leading to obstruction.
Terminology
SMA syndrome should not be confused with nutcracker syndrome (which can be an association), also a superior mesenteric artery compression disorder, where the SMA compresses the left renal vein, although some authors use the terms interchangeably.
Epidemiology
It is an uncommon but a well-recognized clinical entity. About 400 cases have been described in the English literature. It is seen more commonly in females than in males and usually occurs in older children and adolescents.
Clinical presentation
Patients with SMA syndrome may present acutely, with chronic insidious symptomatology, or with an acute exacerbation of chronic symptoms:
- acute presentation is usually characterized by signs and symptoms of duodenal obstruction
- chronic cases may present with long-standing vague abdominal symptoms, early satiety and anorexia, or recurrent episodes of abdominal pain, associated with vomiting
Pathology
Fat and lymphatic tissues around the SMA provide protection to the duodenum against compression. Under conditions of severe weight loss, this cushion around the SMA is diminished, causing angulation and reduction in the distance between the aorta and the superior mesenteric artery. This is usually associated with conditions causing significant weight loss such as:
- anorexia nervosa
- malabsorption
- hypercatabolic states (burns, major surgery, malignancy)
- severe congestive heart failure causing cachexia
Other conditions may also precipitate this syndrome:
- increased spinal lordosis
- application of a body cast
- short ligament of Treitz
- multiple attachments of the ligament of Treitz to the duodenum
- high fixation of the duodenum by the ligament of Treitz
- unusually low origin of SMA
- an anomalous SMA crossing directly over the aorta
- associated with diabetes mellitus and blunt abdominal trauma
Radiographic features
The diagnosis of SMA syndrome is based on clinical symptoms and radiologic evidence of obstruction.
Plain radiograph
The stomach and proximal duodenum are dilated, and filled with gas and/or fluid.
Fluoroscopy
Upper GI fluoroscopy can demonstrate dilatation of the first and second part of the duodenum, extrinsic compression of the third part, and a collapsed small bowel distal to the crossing of the SMA.
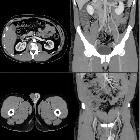
CT/MRI
CT and magnetic resonance angiography (CTA/MRA) enable visualization of vascular compression of the duodenum and measurement of aortomesenteric distance:
- normally, the aortomesenteric angle and aortomesenteric distance are 28-65° and 10-34 mm, respectively.
- in SMA syndrome, both parameters are reduced, with values of 6° to 22° and 2 to 8 mm.
History and etymology
SMA syndrome was first described by Baron Carl von Rokitansky (1804-1878), Bohemian pathologist, in 1861. Later, Sir David Percival Dalbreck Wilkie (1882-1938), English surgeon, provided a more detailed clinical and pathophysiologic description in a series of 75 patients in 1927 and suggested treatment approaches .
Treatment and prognosis
Traditionally, treatment has consisted of conservative measures such as:
- start with the medical management, first which include decompression of the stomach and duodenum with a nasogastric tube, correction of nutritional and electrolytes deficiencies, through TPN, or preferably, if possible, enteral feeding with a nasojejunal tube past the point of compression, which fulfills nutritional requirements while avoiding the complications of TPN. When tolerated, oral feeding may be resumed. This helps build up the fat cushion between the SMA and aorta and, hence, may help in reversing the situation.
- posturing maneuvers during meals and motility agents may be helpful in some patients
- lying in right decubitus position may relieve compression of duodenum
Surgery may be considered if conservative treatment fails:
- duodenojejunostomy is effective in the majority of patients
- laparoscopic duodenojejunostomy offers a new minimally invasive therapeutic approach to SMA syndrome
- laparoscopic surgery involving lysis of the ligament of Treitz with the mobilization of the duodenum is another minimally invasive approach
Differential diagnosis
Other disorders which can present in a similar manner include:
- diabetic gastroparesis
- scleroderma with duodenal involvement
- hereditary megaduodenum
- megaduodenum due to aganglionosis.
The distinction between these entities and SMA syndrome is important, particularly if surgical intervention is being considered.
Siehe auch:
- Truncus-coeliacus-Kompressionssyndrom
- Duodenum
- Arteria mesenterica superior
- Nussknacker-Syndrom
- vaskuläre Kompressionssyndrome
- Retentionsmagen
- Vena-mesenterica-superior-Syndrom
und weiter:


 Assoziationen und Differentialdiagnosen zu Arteria-mesenterica-superior-Syndrom:
Assoziationen und Differentialdiagnosen zu Arteria-mesenterica-superior-Syndrom: