bronchial atresia























Bronchial atresia is a developmental anomaly characterized by focal obliteration of the proximal segment of a bronchus associated with hyperinflation of the distal lung.
On imaging, it commonly presents as a proximal focal tubular-shaped opacity radiating from the hilum associated with a distal area of hyperlucent lung parenchyma.
Clinical presentation
Bronchial atresia is usually asymptomatic and may be found incidentally. If symptomatic, it may cause shortness of breath, cough, or rare infection.
Pathology
The exact cause of bronchial atresia is not well known. Focal bronchial interruption appears to occur before birth. As the bronchial pattern is entirely normal distal to the site of stenosis, it has been suggested that atresia is probably secondary to a traumatic event during fetal life rather than a result of abnormal growth and development .
The bronchi distal to the atresia become filled with mucus and may form a mucocoele/bronchocoele. The lung distal to the atretic bronchus develops normally but is overinflated due to collateral air drift with air trapping.
Location
It is typically at the segmental or subsegmental level. It can involve any lobe but most commonly occurs at the apicoposterior segment of the left upper lobe,followed by the right upper lobe .
Radiographic features
Plain radiograph
It usually presents as a proximal focal ovoid or tubular opacity (finger-in-glove) radiating from the hilum associated with a distal area of hyperlucent lung.
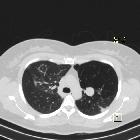
CT
- atretic bronchial stump(s) often become(s) plugged with mucus and can give a finger-in-glove appearance
- distal lung parenchyma supplied by the atretic segment can be hyperlucent due to oligemia and air trapping with air entering through pores of Kohn
Treatment and prognosis
HRCT features are usually typical but segmental resection may be done in certain cases to rule out a rare possibility of underlying small malignancy as the cause of obstruction .
Complications
Although it is usually an incidental finding, it may be associated with recurrent infections in 20% of patients.
History and etymology
It is thought to have been first described in 1953 by Ramsay et al. in a series of patients with cystic lung disease.
Differential diagnosis
- congenital lobar emphysema (CLE)
- opacities are only seen in the immediate postnatal period in a diffuse pattern related to fluid retention
- congenital pulmonary airway malformation (CPAM)
- allergic bronchopulmonary aspergillosis (ABPA)
- for finger-in-glove appearance
- bronchogenic cyst
- usually not associated with hyperlucent lung, unless causing bronchial compression
- pulmonary sequestration
- radiographs will often show an opacity in the affected segment
- it usually affects lower lobes rather than upper lobes
- scimitar syndrome
- small lung with ipsilateral mediastinal shift rather than focal hyperinflation
- tubular structure paralleling the right heart border in the shape of a Turkish sword (“scimitar”)
- endobronchial tumor (e.g. carcinoid)
Siehe auch:
- Allergische bronchopulmonale Aspergillose
- kongenitales lobäres Emphysem
- bronchiales Karzinoid
- kongenitale Anomalien des Tracheobronchialsystems
- Trachealatresie
und weiter:


 Assoziationen und Differentialdiagnosen zu Bronchialatresie:
Assoziationen und Differentialdiagnosen zu Bronchialatresie:



