Steißbeinteratom

















Sacrococcygeal teratoma (SCT) refers to a teratoma arising in the sacrococcygeal region. The coccyx is almost always involved .
Epidemiology
It is the commonest congenital tumor in fetus and neonate . The incidence is estimated at ~1:35000-40000. There is recognized female predilection with a M:F ratio of 1:4. The sacrococcygeal region is the commonest location for non-CNS teratomas.
Clinical presentation
Presentation varies depending on if a tumor has an intrapelvic location or has an extra-fetal extension (see further classification below). Intrapelvic tumors can manifest after birth with genitourinary and gastrointestinal symptoms given the compression of those structures.
Pathology
They are thought to arise from totipotent cells from the node of Hensen at the anterior aspect of the coccyx by about the 2 to 3 weeks of gestation. They are most often mixed solid/cystic, although purely cystic types can occur in ~15% of cases.
A tumor is composed of all three germ cells (i.e. ectoderm, mesoderm and endoderm).
Genetics
- most cases tend to be sporadic
Associations
Markers
Can have elevated levels of:
- alpha-fetoprotein (AFP)
- beta HCG
Classification
A pathology-based classification is as:
- benign (mature): much more common, comprising ~ 60-70%
- malignant (immature)
A location-based classification system according to the American Academy of Pediatric Surgery Section Survey is:
- type I: developing only outside the fetus (can have small pre-sacral component); accounts for the majority of cases, 47%
- type II: extra-fetal with intrapelvic presacral extension
- type III: extra-fetal with extension through pelvis into abdomen
- type IV: tumor developing entirely in the fetal pelvis
Radiographic features
Plain radiograph
- may show a large mass projecting from the lower pelvic region or within the abdominopelvic cavity
- may show calcification
CT
Not part of a routine investigation. Identifies bone, fat and cystic components. Calcification may again be seen.
Ultrasound
Mature types tend to be more cystic which show as anechoic components. Solid types (which are much rarer) often show an echogenic mass within the pelvis.
The correlation between sonographic appearances and malignant components are thought to be poor .
Color Doppler interrogation in some tumors may show marked hypervascularity with arteriovenous (AV) shunting.
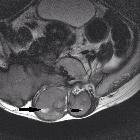
MRI
Superior to ultrasound especially in the assessment of the following areas :
- colonic displacement
- ureteric dilatation
- associated hip dislocation
- intraspinal extension
- vaginal dilatation
- metastatic assessment in malignant lesions
Signal characteristics can significantly vary depending on the constituent of the teratoma .
- T1: fat components appear high signal, calcific/bony components low signal
- T2: fluid (cystic) components appear high signal, calcific bony components low signal
- T2* GRE: magnetic susceptibility artefact because of calcifications
- T1 C+ (Gd): enhancing solid components
Treatment and prognosis
An SCT can be benign or malignant depending on whether mature or immature. The majority, however, tend to be benign (~80% ). Those presenting in older infants tend to have a higher malignant potential which those presenting in utero have a poor prognosis due to complications. Malignant change may be also commoner in males. Treatment is with surgical excision inclusive of coccygectomy with additional chemotherapy for malignant tumors .
Complications
- high output cardiac failure from AV shunting: which in turn can cause hydrops fetalis
- ureteric obstruction
- gastrointestinal tract obstruction
- compression of underlying nerves: giving urinary/fecal incontinence
- anemia
- dystocia
- tumor rupture
Differential diagnosis
General imaging differential considerations include:
- sacral chordoma
- terminal myelocystocoele: for cystic types on ultrasound
- sacral meningocele
For type IV lesions also consider:
- low-lying neuroblastoma
- low-lying rhabdomyosarcoma
- small round blue cell tumor in the sacral region
- enteric (tailgut) cyst: for a purely cystic SCT
Siehe auch:
- Ependymom
- Teratom
- Neuroblastom
- Rhabdomyosarkom
- Neurofibrom
- Myelomeningozele
- benignes Ganglioneurom
- Fibrosarkom
- Riesenzelltumor des Sakrums
- sacrococcygeales Chordom
- kindlicher präsakraler Tumor
- Rektumduplikatur
- enteric (tail gut) cyst
- enterogene Zyste
- small round blue cell tumour
und weiter:


 Assoziationen und Differentialdiagnosen zu Steißbeinteratom:
Assoziationen und Differentialdiagnosen zu Steißbeinteratom: