Inferior vena cava leiomyosarcoma





















Inferior vena cava leiomyosarcomas are the most common type of retroperitoneal leiomyosarcoma and most common primary malignancy of the inferior vena cava.
Epidemiology
Three-quarters of cases occur in women, usually aged 40-60 years .
Clinical presentation
When symptomatic, patients most commonly present with abdominal pain or distension . A minority of patients present with lower extremity deep venous thrombosis .
Pathology
Leiomyosarcomas of the inferior vena cava are slow-growing malignancies .
Etiology
As with other leiomyosarcomas, the histologic origin is smooth muscle cells. These are present in the vessel wall.
Location
The tumors may be classified by the segment of inferior vena cava they involve, which carries implications for surgical planning and prognostication :
- hepatic (6-24%)
- renal and suprarenal (42-50%)
- infrarenal (34-44%)
Metastatic disease occurs in up to half of cases at presentation, most commonly involving liver, followed by lung .
Radiographic features
The tumor may be intraluminal, extraluminal, or both . The presence of a tumor limited to and expanding the inferior vena cava is most likely an inferior vena cava leiomyosarcoma .
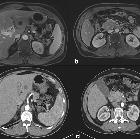
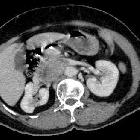
CT
After identifying a retroperitoneal mass that contacts the inferior vena cava, CT features may help distinguish the origin :
- in inferior vena cava leiomyosarcomas, the inferior vena cava wall is usually imperceptible at the point of maximal contact with the mass
- in other retroperitoneal tumors, the inferior vena cava is usually compressed at the perimeter of the mass (negative embedded organ sign)
On contrast-enhanced CT, if the tumor has an intraluminal component, it appears as a heterogeneously enhancing filling defect in the inferior vena cava .
For tumors with an extraluminal component, CT-guided core needle biopsy is typically employed to obtain tissue and establish the diagnosis .
Angiography
For intraluminal tumors, venography may show obstruction of the inferior vena cava and presence of collateral veins . The tumor itself demonstrates neovascularity with marked parenchymal tumor blush .
For tumors with predominantly intraluminal growth, transvenous biopsy is a feasible alternative to percutaneous biopsy .
MRI
Signal characteristics depend on the degree of necrosis, which appears low intensity on T1-weighted images and high intensity on T2-weighted images .
In contrast to bland thrombus, intraluminal leiomyosarcoma tumor thrombus appears iso- to hyperintense on T2-weighted images, enhances on T1-weighted postcontrast images, and expands the lumen .
Treatment and prognosis
The treatment includes surgical resection, most commonly with inferior vena cava ligation and primary/patch repair . The prognosis is poor. Recurrence affects half of the patients and the 5-year survival is 33% .
The best prognosis is associated with tumors in the renal and suprarenal inferior vena cava, while the worst prognosis is associated with tumors in the hepatic segment of the inferior vena cava .
Differential diagnosis
Intraluminal tumor should be distinguished from bland thrombus (inferior vena cava thrombosis).
The differential includes other less common retroperitoneal mesenchymal neoplasms that may involve the inferior vena cava:
Involvement of adjacent organs should be identified, raising the more likely possibility of tumor thrombus extending from those organs into the inferior vena cava:
- cardiac angiosarcoma
- hepatocellular carcinoma
- adrenal cortical carcinoma
- renal cell carcinoma (most common)
- uterine leiomyosarcoma and intravenous leiomyomatosis
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Leiomyosarkom der Vena cava inferior:
Assoziationen und Differentialdiagnosen zu Leiomyosarkom der Vena cava inferior: