acute otomastoiditis

















Acute mastoiditis refers to a suppurative infection of the mastoid air cells. It is the most common complication of acute otitis media.
Terminology
In acute otitis media, an inflammatory middle ear effusion is present that can freely move into the mastoid air cells. Consequently, some authors comment that a mild mastoiditis is technically present in nearly all cases of acute otitis media . The mere presence of mastoid fluid on imaging, however, does not change the management of otherwise uncomplicated acute otitis media. Thus, many clinicians reserve the diagnosis for when there are clinical signs or symptoms of inflammation involving the mastoid. When mastoiditis and acute otitis media occur concurrently, sometimes the term acute otomastoiditis is used.
When there is clinical evidence of acute mastoiditis, the initial stage is referred to as acute mastoiditis with periostitis, incipient mastoiditis, or mild mastoiditis . When mucoperiosteal involvement evolves into resorption of mastoid bony septa, this stage is referred to as coalescent mastoiditis. Coalescent mastoiditis is a radiological diagnosis.
Epidemiology
Acute mastoiditis, like acute otitis media, is largely a disease of childhood.
Clinical presentation
Acute mastoiditis characteristically presents with postauricular tenderness, erythema, and swelling causing protrusion of the auricle. Common non-specific findings include otalgia and fever. Abscess may present with fluctuance or a palpable mass.
Complications
- subperiosteal abscess
- Bezold abscess
- Citelli abscess
- labyrinthitis
- petrous apicitis: extension of infection into a pneumatized petrous apex; ~30% of the population has pneumatized petrous apex
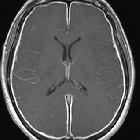
- intracranial extension
- epidural abscess, most commonly perisinus (adjacent to sigmoid sinus)
- meningitis
- subdural empyema
- cerebral abscess
- dural sinus occlusive disease (DSOD)
- facial nerve dysfunction
- thrombosis of mastoid emissary vein (Griesinger sign)
Pathology
Acute mastoiditis with periostitis is pathologically characterized by spread of infection through the mastoid emissary veins into the periosteum. Acute coalescent mastoiditis is characterized by infiltration and destruction of the bone, essentially osteomyelitis.
It is most frequently due to bacterial infections, with Streptococcus pneumoniae and Haemophilus influenzae accounting for 65-80% of cases.
H. influenzae, although less common, is the more aggressive agent, more frequently resulting in complications, especially meningitis.
Etiology
- Streptococcus pneumoniae: most common
- Haemophilus influenzae: common and more aggressive than pneumococcus
- Aspergillus: aggressive; seen in older patients; frequently associated with facial nerve dysfunction
- tuberculous otomastoiditis: increasing frequency due to greater immunocompromised population
Radiographic features
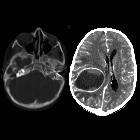
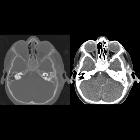
CT is the initial investigation of choice. Post-contrast imaging is helpful in assessing for associated soft tissue or intracranial complications.
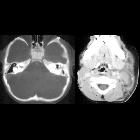
CT
- partial-to-complete opacification of the mastoid air cells, which is non-specific but supportive of incipient mastoiditis in the appropriate clinical setting
- erosion of mastoid air cell bony septa, which establishes the diagnosis of coalescent mastoiditis
- erosion of the lateral wall of the mastoid, suggestive of subperiosteal abscess, or of the sigmoid plate, suggestive of epidural abscess
- mass with surrounding fat stranding or rim-enhancing collection deep to the sternocleidomastoid muscle, suggestive of Bezold abscess, or within the digastric triangle, suggestive of Citelli abscess
- erosion indicating osteomyelitis of the petrous apex (petrous apicitis, petrositis) or occipital bone (confusingly also known as Citelli abscess)
- cerebral abscess
- dural venous sinus thrombosis
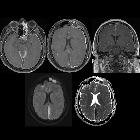
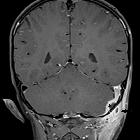
MRI
- partial-to-complete opacification of the mastoid air cells +/- middle ear cleft
- fluid signal intensity in the mastoid should not be interpreted as mastoiditis without other evidence, such as mucosal contrast enhancement and/or diffusion restriction
Signal characteristics
Typical findings in mastoiditis include :
- T1: low signal
- T2: high signal
- DWI/ADC: diffusion restriction may be present
- T1 C+: mucosal contrast enhancement is present in the majority
Treatment and prognosis
Usually, antibiotics are all that is required for treatment.
See also
Siehe auch:
- Hirnabszess
- chronische Otomastoiditis
- Meningitis
- subdurales Empyem
- Mastoiditis
- Labyrinthitis
- aspergillus
- subperiosteal abscess (mastoid)
- einschmelzende Mastoiditis
- Pyramidenspitzen-Osteomyelitis
- tuberkulöse Otomastoiditis
- otoastoiditis
und weiter:


 Assoziationen und Differentialdiagnosen zu akute Otomastoiditis:
Assoziationen und Differentialdiagnosen zu akute Otomastoiditis: