petrous apicitis




Petrous apicitis, also known as apical petrositis, is infection with involvement of bone at the very apex (petrous apex) of the petrous temporal bone.
Epidemiology
Petrous apicitis is less common than it once was, on account of the widespread and early use of antibiotics for acute otomastoiditis .
Clinical presentation
Clinical presentation depends on whether petrous apicitis is isolated or (as is more common) is a complication of acute otomastoiditis. In the latter, symptoms will be those of a middle ear infection, superimposed on symptoms specific to petrous apicitis :
- deep facial pain due to inflammation of the adjacent dura and trigeminal nerve in Meckel's cave
- abducens nerve palsy (see Gradenigo syndrome) due to involvement of Dorello's canal
Gradenigo syndrome is the classical presentation of petrous apicitis, but it is not present in all patients . Extension of infection to involve the petrous apex should be suspected in all patients with signs and symptoms of acute otomastoiditis and deep ipsilateral pain .
Presentation may also be due to extension of inflammatory/infective changes beyond the petrous apex.
- dural venous sinus thrombosis
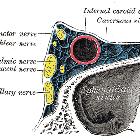
- cavernous sinus thrombosis
- sigmoid sinus thrombosis
- jugular vein thrombosis
- intracranial extension
- frank meningitis: Proteus, Pseudomonas and Staphylococcus species are usually implicated
- epidural abscess
- subdural empyema
- cerebral abscess
Pathology
There is debate as to whether it represents osteomyelitis in non-pneumatized bone, or whether (and more generally accepted) a form of osteitis developing from infected and obstructed air cells in a pneumatized petrous apex (analagous to coalescent mastoiditis) . Approximately 30% of the population has a pneumatized petrous apex , but it is frequently asymmetric.
Radiographic features
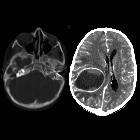
CT
CT is the modality of choice to evaluate bony changes in the temporal bone, which in the setting of petrous apicitis are erosive lysis with ill-defined irregular edges. Contrast enhanced scans may demonstrate peripheral enhancement as well as dural thickening and enhancement, although these are better appreciated on MRI.
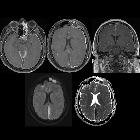
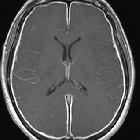
MRI
MRI is more sensitive in detecting dural thickening and enhancement as well as leptomeningitis, cerebritis and cerebral abscess.
Findings are those of fluid signal with the petrous apex often with peripheral enhancement, which presumably represents a combination of residual mucosa, granulation tissue and adjacent dura/periosteum . Thus:
- T1: fluid signal (low to intermediate)
- T2: fluid signal (hyperintense)
- T1 C+ (Gd): peripheral enhancement
Thickening of the dura of Meckel's cave and the cavernous sinus should be sought, as well as for the findings of cavernous sinus thrombosis.
Treatment and prognosis
In many instances treatment with appropriate intravenous antibiotics suffices. In more severe cases surgical drainage may be required .
Differential diagnosis
On imaging consider
- cholesterol granuloma
- congenital cholesteatoma
- glomus jugulare
- mucocoele of the petrous apex: uncommon
- base of skull tumors
- metastasis
- chondrosarcoma
- chordoma
Siehe auch:
- Osteomyelitis
- Nervus trigeminus
- Cholesterolgranulom der Felsenbeinspitze
- Läsionen der Felsenbeinspitze
- Chondrosarkom
- Sinusthrombose
- Hirnabszess
- Chordom
- Glomus jugulare Tumor
- Meningitis
- Mucocele
- subdurales Empyem
- akute Otomastoiditis
- Nervus abducens
- Gradenigo-Syndrom
- congenital cholesteatoma
- Flüssigkeit im Apex petrosus
- Cholesteatom der Felsenbeinspitze
- einschmelzende Mastoiditis
- Sinus cavernosus Thrombose
- dorello's canal
und weiter:


 Assoziationen und Differentialdiagnosen zu Pyramidenspitzen-Osteomyelitis:
Assoziationen und Differentialdiagnosen zu Pyramidenspitzen-Osteomyelitis: