cavernous sinus thrombosis



Cavernous sinus thrombosis (CST) is a rare condition, most commonly infectious in nature, and the diagnosis on imaging is not always straightforward. It has high mortality and morbidity rates.
Epidemiology
Cavernous sinus thrombosis is rare with ~4.5 cases per 1,000,000 per year . It is the least common dural venous sinus thrombosis, accounting for <1.5% of cases .
Clinical presentation
A headache is the most common symptom (85%). Focal neurological signs and/or seizures may also occur . Isolated CN III palsy is thought to be an early manifestation.
Orbital signs can include:
- chemosis/periorbital swelling
- exophthalmos
Pathology
Etiology
- contiguous spread of infection, typically Staphylococcus aureus (~55%):
- paranasal sinuses
- middle third of the face
- dental abscess or orbital cellulitis (less common)
- cavernous sinus compression, e.g. trauma, tumor
- thrombophilic conditions, e.g. protein C/S deficiency, oral contraceptive use, malignancy, pregnancy
- idiopathic (25%)
The cavernous sinus drains the superior and inferior ophthalmic veins and superficial cortical veins anteriorly . Cavernous sinus thrombosis from a septic etiology occurs due to embolization of bacteria which trigger thrombosis that becomes trapped within the cavernous sinus. The subsequent reduction in venous drainage results in facial and periorbital edema, ptosis, proptosis, chemosis, painful eye movements, papilledema, retinal venous distension and loss of vision .
Thrombus can propagate into the dural system as the lack of valves in the dural sinus allow flow through emissary veins into and out of the cavernous sinus .
Radiographic features
Cavernous sinus thrombosis is a clinical diagnosis. MRI with contrast is the imaging modality of choice to confirm its presence and to differentiate it from alternatives such as orbital cellulitis, which may have a similar clinical presentation.
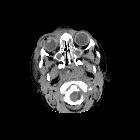
CT
- non-contrast: high-density thrombus in affected cavernous sinus (seen in only 25%)
- contrast-enhanced: distended cavernous sinus with a non-fat density filling defect
MRI
- T1 and T2
- absent flow void
- signal characteristics vary depending on the age of the thrombus but will be abnormal
- contrast-enhancement or lack of is not a reliable indicator as organizing thrombus can enhance
- diagnosis can generally be made on MR venography
Treatment and prognosis
Primary consideration for the management of cavernous sinus thrombosis is the use of antimicrobials and antithrombotic agents . The mortality rate is up to 30%. Significant morbidity (e.g. blindness, cranial nerve palsy) in survivors not uncommon .
Complications
As the dural venous and cavernous systems are valveless, communication between dural sinuses and cerebral and emissary veins can lead to meningitis, dural empyema or cerebral abscess . Propagation of infection via the internal jugular vein can result in septic pulmonary emboli, pulmonary abscess, pneumonia or empyema. Compression of the internal carotid artery and pituitary gland may result in stroke and hypopituitarism respectively .
Differential diagnosis
Consideration is given to other causes of cavernous sinus syndrome and painful ophthalmoplegia caused by local compression of which 30% are tumors :
- carotid-cavernous fistula
- superior orbital fissure syndrome
- meningioma
- Tolosa-Hunt syndrome
- lytic bone lesions
- cavernous hemangioma
Practical points
The dural venous sinuses and cerebral veins should also be carefully evaluated in cases of cavernous sinus thrombosis as up to 90% of patients will have multiple thromboses .
Siehe auch:
- Orbitaphlegmone
- Vena ophthalmica superior
- Carotis-Sinus-cavernosus-Fistel
- Pyramidenspitzen-Osteomyelitis
und weiter:


 Assoziationen und Differentialdiagnosen zu Sinus cavernosus Thrombose:
Assoziationen und Differentialdiagnosen zu Sinus cavernosus Thrombose: