Adenokarzinom der Harnblase





Adenocarcinoma of the urinary bladder is rare and accounts for only ~1% of all bladder cancers (90% are transitional cell carcinomas).
Pathology
Metaplasia of urinary bladder induced by chronic irritation or infection can lead to adenocarcinoma. Pathological types of adenocarcinoma of the urinary bladder are:
- mucinous adenocarcinoma
- signet-ring type
- papillary adenocarcinoma
- not otherwise specified (NOS)
Bladder adenocarcinoma may be subclassified as primary (two-thirds are non-urachal and one-third are urachal ) or secondary (metastases).
Etiology
- persistent urachal remnant (most common)
- cystitis glandularis (itself secondary to bladder outlet obstruction, chronic infection and/or bladder calculi)
- schistosomiasis (bilharziasis), especially where endemic
- associated with bladder exstrophy
Radiographic features
CT
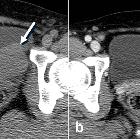
Non-urachal adenocarcinoma
- diffuse bladder wall thickening
- stranding of perivesical fat
- regional lymphadenopathy
- invasion of rectus muscles
Urachal adenocarcinoma
- characteristically in the midline at the dome of the bladder, or along the course of urachus (from the bladder to umbilicus)
- a midline, infraumbilical soft tissue mass with peripheral calcification is characteristically urachal adenocarcinoma unless proven otherwise (calcification in 70% of cases)
- usually large tumors (5-6 cm) with prominent extravesical component
- mixed solid-cystic appearance in most cases
MRI
Solid components of the tumor are isointense, while cystic mucinous component appears hyperintense on T2W images. Localizing a urachal carcinoma may be easier on the sagittal images.
Treatment and prognosis
Due to their extravesical location, urachal carcinomas present very late and thus carry a poor prognosis. Radical cystectomy is considered the treatment of choice. However, en bloc resection of the extravesical component, adjacent peritoneum and the abdominal wall is also needed.
Siehe auch:
- Urachusrest
- cystitis glandularis
- Urothelkarzinom
- Blasenekstrophie
- Harnblasenkarzinom
- Urachuskarzinom
- Plattenepithelkarzinom der Harnblase
und weiter:


 Assoziationen und Differentialdiagnosen zu Urachuskarzinom:
Assoziationen und Differentialdiagnosen zu Urachuskarzinom: