brainstem glioma





















Brainstem gliomas consist of a heterogeneous group which vary greatly in histology and prognosis.
Terminology
Unless otherwise specified the term brainstem glioma usually refers to the most common histology, the diffuse brainstem glioma, and in children this is most likely a diffuse midline glioma H3 K27M–mutant.
Epidemiology
Brainstem gliomas account for ~25% of all posterior fossa tumors and are most common in children between 7 and 9 years of age . There is no recognized gender or racial predilection.
Brainstem gliomas are also recognized in adults, although they are rare accounting for only 2% of adult brain tumors . They typically occur in younger adults (third and fourth decade) and tend to be of low grade (WHO I or II) .
Clinical presentation
Although the exact presentation will vary according to location and size of the tumor, in general patients will exhibit a combination of :
- ataxia
- cranial nerve palsies
- long tract signs
- hydrocephalus
The duration of symptoms is usually much shorter in diffuse gliomas, in which the history is typically very short (a few days) . Additionally, diffuse gliomas more frequently have multiple cranial nerve palsies.
Pathology
Histology
Recognized histological types include:
- diffuse astrocytoma
- usually diffuse midline glioma H3 K27M–mutant (WHO grade IV)
- other tumors also encountered (WHO grades II-IV)
- focal glioma
- fibrillary astrocytoma (grade II): most common histology
- pilocytic astrocytoma
- ganglioglioma
- (dorsally) exophytic glioma
- Low-grade astrocytoma
- ganglioglioma
- NF1 associated brainstem glioma
- seen in up to 9% of NF1 patients
- most frequently seen in the medulla
- appears similar to a sporadic focal brainstem glioma but has an even better prognosis, with little if any progression
Classification
The most frequently used classification system is to divide these tumors into four types :
- tectal plate glioma
- other focal gliomas
- probably an artificial group made up of the downward extension of true brainstem gliomas or upward extension of upper cervical cord intramedullary spinal cord tumors
Associations
Location
As a general rule mesencephalic tumors tend to be of a lower grade than those in the pons and medulla .
- pontine
- most common location
- classic location for the childhood 'brainstem glioma' which tends to refer to a diffuse pontine glioma, the majority of which are diffuse midline gliomas, H3 K27M–mutant
- focal dorsally exophytic brainstem glioma is an uncommon variant accounting for only 10% of pontine tumors, and has a much better prognosis, as it usually represents a pilocytic astrocytoma
- overall survival of pontine gliomas is 10% at 5 years
- mesencephalic
- includes diffuse, focal, exophytic and tectal variants.
- focal brainstem gliomas are more common here than elsewhere in the brainstem
- tectal plate gliomas are typically indolent
- medullary
- least common location
- includes focal dorsally exophytic, focal, diffuse and cervicomedullary junction variants
- cervicomedullary junction tumors usually represent upper cervical tumors extending superiorly
- most common location for NF1 associated tumors
Radiographic features
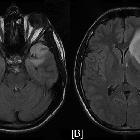
MRI
MRI is the imaging modality of choice. The appearance will vary with the tumor type, thus please refer to individual articles.
DSA/angiography
May show anterior displacement of the basilar artery.
Treatment and prognosis
Again, both treatment and prognosis are significantly influenced by tumor type, morphology and location. Radiation is a key part of treatment.
As a general rule, dorsal exophytic tumors and cervicomedullary tumors tend to do best with surgery, whereas surgery has no role in the management of diffuse brainstem gliomas.
Prognosis
- diffuse
- terrible prognosis
- 90-100% patients die within 2 years of diagnosis
- focal (tectal glioma)
- excellent long-term survival with CSF shunting (essentially benign lesions)
- focal (other)
- good long-term prognosis with surgery
- (dorsally) exophytic tumors
- good long-term prognosis with surgery
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Hirnstammgliom:
Assoziationen und Differentialdiagnosen zu Hirnstammgliom: