CNS Lymphoma

MR imaging
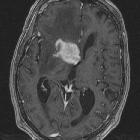
features of intracranial primary CNS lymphoma in immune competent patients. Axial post-contrast T1WI shows a slit-like center (white arrow) in an otherwise intensely, solidly contrast-enhancing mass in the right frontal white-matter. The mass causes little mass-effect relative to its large size.

MR imaging
features of intracranial primary CNS lymphoma in immune competent patients. Axial post-contrast T1WI shows a subcortical lesion with two deep indentations reflecting the overlying sulci (two overlapping crescents).

MR imaging
features of intracranial primary CNS lymphoma in immune competent patients. Axial T2WI, T1WI and contrast-enhanced T1WI as well as ADC and DWI maps show the classic appearance of PCNSL where the mass is isointense to mildly hypointense on T2WI and isointense on T1WI (relative to gray-matter) and shows predominantly solid, intense contrast enhancement (1a-1d). The mass is also in a typical distribution abutting a CSF-containing space (in the splenium of the corpus callosum abutting the lateral ventricles in this case). The mass is associated with extensive perilesional T2-hyperintensity. On ADC and DWI, the mass shows diffusion restriction.

MR imaging
features of intracranial primary CNS lymphoma in immune competent patients. Post-contrast T1WI in the axial, coronal and sagittal planes show two intensely, solidly contrast-enhancing masses (2a-2c). The larger one involves the hypothalamus and optic chiasm as well as the pituitary gland. The other one is subcortically located in the left temporal lobe.

MR imaging
features of intracranial primary CNS lymphoma in immune competent patients. Axial pre-contrast T1WI shows a hyperintense mass in the right temporal lobe.

MR imaging
features of intracranial primary CNS lymphoma in immune competent patients. Axial post-contrast T1WI and cerebral blood volume color map from perfusion exam show the reduced cerebral blood volume values in the tumor (6a-b).

Spectrum of
imaging findings in AIDS-related diffuse large B cell lymphoma. Axial CT image (a) demonstrates bilateral axillary lymphadenopathy, proven to be DLBCL after biopsy. The patient successfully completed treatment but developed CNS symptoms 1 year later. MRI of the brain (b) showed a large heterogenous mass in the left cerebral hemisphere which biopsy was proven to be lymphoma. A previous MRI brain (c) was negative for CNS involvement

Magnetic
resonance imaging of sellar and juxtasellar abnormalities in the paediatric population: an imaging review. Leptomeningeal spread of lymphoma. Sagittal post contrast T1WI demonstrates diffuse intracranial and spinal leptomeningeal enhancement in a 22-month-old infant boy with lymphoma including the sella and parasellar subarachnoid space

Primary
central nervous system small lymphocytic lymphoma in the bilateral ventricles: two case reports. The solid lesions in the bilateral ventricles presenting as isointense on T1WI (a, white arrow) and hypointense on T2WI and FLAIR images (b and c, white arrow). Striking contrast enhancement (d-f, axial (white arrow), sagittal, and coronal T1 with contrast) and hyperperfusion are demonstrated in the lesions of the bilateral ventricles (g and h, white arrow, rCBF, rCBV map). MRS from the lesion demonstrates a high Cho peak and a low NAA peak with a Cho/NAA ratio of 3.85 (i and j). CSF cytology reveals malignant cells (k)

Primary
central nervous system small lymphocytic lymphoma in the bilateral ventricles: two case reports. The solid lesions are located in the bilateral ventricles and fornix, presenting as isointense on T1WI (a, white arrow) and hypointense on T2WI (b, white arrow) without restricted diffusion (c, white arrow on DWI). Axial SWI demonstrates enlarged veins in the thalamus and located adjacent to the lateral ventricles (d). The lesions demonstrate homogeneous contrast enhancement (e-g, axial (white arrow), sagittal, and coronal T1 with contrast) and hyperperfusion on 3D-ASL MR perfusion imaging (h, black arrow). Open biopsy of the lesions shows diffuse proliferating small lymphocytes (H&E × 200) (i). CD-20 positivity of lymphocytes (× 200) (j). CSF cytology reveals malignant cells, and flow cytometry immunophenotyping reveals a lymphocyte subset with the profile of CD19+ (50.81%) (k and l)

Zerebrale und
zerebelläre Mitbeteiligung bei ansonsten mediastinalem Lymphom: Obere Reihe T2, DWI, T1 nativ, FLAIR sagittal, untere Reihe Petit, ADC, T1 KM axial und sagittal.
CNS lymphoma refers to the involvement of the central nervous system with lymphoma. It can be broadly divided into primary and secondary, with a number of special types of also recognized.
- primary CNS lymphoma (PCNSL)
- secondary CNS lymphoma
- parenchymal
- leptomeningeal
Note that this is a simplified version of the current WHO classification of CNS tumors, which divides CNS lymphoma into a larger number of subtypes.
Siehe auch:
und weiter:
- verdickter Hypophysenstiel
- Tuberkulose des ZNS
- intraventrikuläres Meningeom
- zerebrale Kryptokokkose
- Hirntumoren
- Tumefaktive Multiple Sklerose
- tumefaktive Demyelinisierung
- hypertrophe Pachymeningitis
- Tuberkulom des ZNS
- Lymphom des spinalen Myelons
- boomerang sign
- primary spinal lymphoma
- intraventricular B cell lymphoma
- pineal lymphoma
- Burkitt-Lymphom des ZNS
- primary CNS lymphoma: involving the septum pellucidum
- zerebelläres Lymphom


 Assoziationen und Differentialdiagnosen zu ZNS Lymphom:
Assoziationen und Differentialdiagnosen zu ZNS Lymphom: