Lymphom des spinalen Myelons







Lymphoma of the spinal cord is an uncommon manifestation of lymphoma. Although lymphoma more commonly involves the vertebral body (vertebral body tumors) or epidural compartment, intramedullary lymphoma may rarely occur.
Apparent intramedullary spinal cord lymphoma may often, in fact, represent a secondary invasion of the spinal cord by leptomeningeal disease.
Epidemiology
Intramedullary spinal lymphoma accounts for 3.3% of all CNS lymphoma, which constitutes only 1% of all lymphomas in the body .
The mean age at presentation is 47 years. Females are more commonly affected than males.
Risk factors
Risk factors for developing CNS lymphoma include:
- AIDS
- transplant recipients
- congenital immunodeficiency
- Epstein-Barr virus infection
Clinical presentation
Clinical presentation is similar to that of other intramedullary spinal tumors, with common symptoms being pain, weakness, and sensory changes.
Pathology
Primary lymphoma of the spinal cord is most often predominantly histiocytic or mixed histiocytic and lymphocytic . 85% are non-Hodgkin lymphomas .
The principal microscopic feature is a dense, perivascular, mononuclear infiltrate composed predominantly of large lymphocytes with prominent nucleoli. Most tumors are B-cell derivatives.
Radiographic features
The most common intramedullary location is the cervical cord, followed by the thoracic cord then the lumbar cord . Most are solitary lesions, however, there may be multiple lesions throughout the spinal cord.
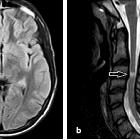
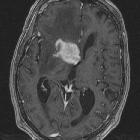
MRI
Although spinal cord expansion is usually present, in some patients there is relatively minimal enlargement of the cord . The lesions are generally poorly defined and tumoral cysts are generally not a feature and secondary syringomyelia is rare . Lymphoma usually does not have a hemorrhagic component .
Reported signal characteristics include:
- T1: isointense to spinal cord
- T2: hyperintense (this is in contrast to the characteristic low T2 signal intensity that is seen in intracranial lesions)
- T1 C+ (Gd): usually solid and homogeneous enhancement
Treatment and prognosis
Radiotherapy is the primary therapy for potential preservation of neurologic function and extension of survival. Minimal data are available on the role of chemotherapy for primary spinal cord lymphoma .
The prognosis for patients with intramedullary spinal lymphoma is poor. The survival rate at 2.5 years is less than 50% .
Differential diagnosis
General imaging differential considerations include:
- spinal astrocytoma
- tumoral cysts are more common
- spinal ependymoma
- tumoral cysts are more common
- hemorrhage is more common
- spinal intramedullary metastases
- usually more sharply circumscribed
- transverse myelitis
- variable contrast enhancement
- rapidly progressive clinical course
- spinal cord contusion
- appropriate history is usually present
- spondylotic myelopathy
- lacks enhancement
- multiple sclerosis with spinal involvement
- most have brain lesions
- typically located eccentrically
- enlargement of the cord is uncommon
- may not demonstrate contrast enhancement
Siehe auch:
- Transverse Myelitis
- Encephalomyelitis disseminata
- primäres ZNS-Lymphom
- neoplasms of the spinal canal
- ZNS Lymphom
- spinales Ependymom
- spinale Metastasen
- spinales Astrozytom
und weiter:


 Assoziationen und Differentialdiagnosen zu Lymphom des spinalen Myelons:
Assoziationen und Differentialdiagnosen zu Lymphom des spinalen Myelons: