Hepatoblastom













Hepatoblastoma is the most common primary malignant liver tumor in children under four years of age who usually present with painless abdominal mass and raised AFP. It is tumor of embryonic origin.
Epidemiology
Most cases are seen during the first 18 months of life and diagnosis in adulthood is exceedingly rare. Occasionally the tumor may be diagnosed antenatally . There is a recognized slight male preponderance with a M:F ratio of up to ≈3:2. There may also be predilection towards the right lobe of the liver.
Clinical presentation
Most children present with abdominal distension or an asymptomatic palpable abdominal mass. However, other presenting symptoms include :
- abdominal pain
- anorexia
- vomiting
- jaundice
- pyrexia
- anemia
- back pain
- pseudo precocious puberty (due to chronic GnRH secretion)
Pathology
Macroscopically hepatoblastomas are usually relatively well circumscribed large masses, usually single, with heterogeneous cut surface .
Histological classification of hepatoblastoma is complicated with multiple subtypes identified. The notable subtypes include:
- epithelial: most common
- fetal: best prognosis
- embryonal
- small cell undifferentiated: worst prognosis
- mixed type: epithelial and mesenchymal. Calcifications are more common in mixed type
It is important to note that with the possible exception of small cell undifferentiated subtype, prognosis is independent of histology when adjusted for stage gender and age .
For full classification please refer to hepatoblastoma histological classification.
Associations
Most hepatoblastomas are seen sporadically, however, it has been known to be associated with:
- Beckwith-Wiedemann syndrome
- hemihypertrophy: seen in 2% of patients with hepatoblastoma
- familial adenomatosis polyposis
- fetal alcohol syndrome
- prematurity and low fetal birth weight
- Gardner syndrome
- glycogen storage disease
- biliary atresia
Markers
Serum alpha fetoprotein (AFP) levels are frequently elevated (90% of cases ).
Staging
Refer to: hepatoblastoma staging.
Caval involvement often indicates unresectable disease.
Radiographic features
Plain radiograph
Abdominal x-rays are nonspecific, typically demonstrating a right upper quadrant mass. Calcifications are visible in 10% of cases .
Ultrasound
On ultrasound, hepatoblastomas appear as predominantly echogenic soft tissue mass. In larger tumors heterogeneity and variable echogenicity is common. Even when large, they tend to be relatively well defined . Intralesional calcifications may be visible as areas of shadowing .
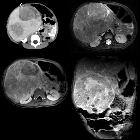
CT
Usually seen as a well defined heterogeneous mass, which is usually hypoattenuating compared to surrounding liver . Frequently there are with areas of necrosis and hemorrhage. Chunky, dense calcifications may be seen in approximately 40% of cases .
CT is also able to evaluate the lungs for metastases and for nodal enlargement.
MRI
MRI is superior to CT in defining tumor margins, vessel involvement and adenopathy .
- T1: generally hypointense
- T1 C+ (Gd): can show heterogeneous enhancement
- T2
- generally hyperintense compared to liver
- areas of necrosis and hemorrhage are common
Angiography
- tend to be hypervascular
Treatment and prognosis
Surgical resection is the treatment of choice although preoperative chemotherapy may be used to reduce tumor bulk. Chemotherapy is also employed in following surgical resections. If the tumor is resectable then liver transplantation provides a cure, as long as no metastatic disease is present. The lungs are a relatively frequent site of metastases.
Overall there is 65-70% long-term survival , however, prognosis depends on staging:
- stage I: can expect very good long-term survival, of up to 100% with combined chemotherapy and surgery
- stage II: 75-80%
- stage III: 65%
- stage IV: 0-27%
Differential diagnosis
General imaging differential considerations include:
- hepatic mesenchymal hamartoma
- infantile hemangioendothelioma
- hepatic metastases, e.g. neuroblastoma
- hepatocellular carcinoma
- rhabdomyosarcoma of biliary tract (rare)
Siehe auch:
- hepatozelluläres Karzinom
- Rhabdomyosarkom
- Lebermetastasen
- hepatoblastoma staging
- pädiatrische Lebertumoren
- Leberhämangiom bei Kindern
und weiter:
- verkalkte Leberläsionen
- Beckwith-Wiedemann-Syndrom
- Proteus-Syndrom
- Abernethy malformation
- altered alpha fetoprotein levels
- Lebertumoren
- small round blue cell tumours
- malignant liver tumours (paediatric)
- fetale Tumoren
- mesenchymales Leberhamartom
- Lebertumoren mit Verkalkungen
- hepatoblastoma histological classification
- hepatoblastoma: metastatic


 Assoziationen und Differentialdiagnosen zu Hepatoblastom:
Assoziationen und Differentialdiagnosen zu Hepatoblastom:



