Inflammatory cerebral amyloid angiopathy






Inflammatory cerebral amyloid angiopathy is an uncommon cerebral amyloid deposition disease, closely related to the far more common non-inflammatory cerebral amyloid angiopathy, and can present as areas of vasogenic edema.
Terminology
The term "inflammatory cerebral amyloid angiopathy" can be used as an umbrella term encompassing two subtypes: cerebral amyloid angiopathy-related inflammation and amyloid β-related angiitis . However, many authors interchange the terms "cerebral amyloid angiopathy-related inflammation" and "inflammatory cerebral amyloid angiopathy," either encompassing of amyloid β-related angiitis or in distinction to it . Still others refer to only cerebral amyloid angiopathy-related inflammation alone or amyloid β-related angiitis alone without mention of the other.
When the distinction is made, the difference lies in whether the inflammation is perivascular only (cerebral amyloid angiopathy-related inflammation or inflammatory cerebral amyloid angiopathy) or also involves and destroys the vessel wall (amyloid β-related angiitis).
This pathological distinction is not reliably predicted on imaging . It may also be possible that, due to sampling error on biopsy, the pathological diagnosis does not reflect the global picture depicted on imaging . For these reasons, this article does not attempt to distinguish between subtypes and treats the terms interchangably.
Other synonyms used for this entity include cerebral amyloid inflammatory vasculopathy, amyloid angiopathy and granulomatous angiitis of the central nervous system, cerebral amyloid angiitis, primary angiitis of the central nervous system associated with cerebral amyloid angiopathy, and cerebral amyloid angiopathy associated with giant cell arteritis .
Epidemiology
The diagnostic criteria for possible or probable inflammatory cerebral amyloid angiopathy require age ≥40 years . In general, the same patient group affected by cerebral amyloid angiopathy is affected, and thus most patients are elderly, typically 60-80 years of age. However, the average patient is a little younger than in non-inflammatory cerebral amyloid angiopathy and older than those with non-amyloid primary cerebral angiitis .
Clinical presentation
The clinical presentation is usually acute or subacute , but may be chronic. The diagnostic criteria for possible or probable inflammatory cerebral amyloid angiopathy require at least one of the following clinical features that is not directly attributable to an acute intracerebral hemorrhage :
- headache
- decrease in consciousness
- behavioral change
- focal neurological signs and seizures
Some patients also present with hallucinations .
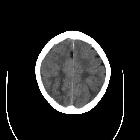
Radiographic features
CT and MRI demonstrate an area of vasogenic edema involving the subcortical white matter . Lesions are usually unifocal but multifocal involvement is occasionally present at the time of diagnosis (~30%) . MRI is the modality of choice in assessing these patients as it is able to visualize the characteristic peripheral microhemorrhages of cerebral amyloid angiopathy.
CT
Subcortical white matter will demonstrate usually a solitary area of low density with localized mass effect .
Angiography (DSA)
Angiography does not reveal evidence of vasculitis involving the large- or medium-sized vessels .
MRI
White matter lesions
The diagnostic criteria for "probable" inflammatory cerebral amyloid angiopathy require white matter hyperintensities on T2-FLAIR that are asymmetric and extend to the immediately subcortical white matter . The asymmetry should not be due to past intracerebral hemorrhage to satisfy this criterion .
The presence of symmetric white matter lesions that extend to the immediately subcortical white matter would only meet criteria for "possible" inflammatory cerebral amyloid angiopathy .
The white matter hyperintensity represents vasogenic edema, which may show localized mass effect. While changes are typically confined to the subcortical white matter, the involvement of the cortex is also encountered and predisposes to seizures .
Hemorrhagic lesions
The diagnostic criteria for both probable and possible inflammatory cerebral amyloid angiopathy require at least one corticosubcortical hemorrhagic lesion , which is best demonstrated as signal loss on T2*-weighted sequences (susceptibility-weighted or gradient echo):
- cerebral macrobleed (intraparenchymal hematoma)
- cerebral microbleed (cerebral microhemorrhage)
- cortical superficial siderosis
In the vast majority of cases (90%), microhemorrhages are present .
Leptomeningeal/vascular involvement
Leptomeningeal contrast enhancement is seen in approximately half of patients . Occasional cases of pathologically-confirmed inflammatory cerebral amyloid angiopathy have been reported with prominent leptomeningeal involvement without the typical white matter or hemorrhagic lesions on imaging . Cases of an isolated leptomeningeal process on imaging are more commonly categorized as amyloid β–related angiitis, within the limitations of variable terminology noted above .
MRA and vessel wall imaging may show medium-sized arteries involved with multifocal stenoses with wall thickening/enhancement . Vessel wall enhancement, however, is not specific for inflammation and may be seen with noninflammatory amyloid angiopathy .
Treatment and prognosis
A significant proportion of patients respond readily to treatment with corticosteroids, with or without a cytostatic agent, with improvement evident within a week or two of commencement of treatment. In fact, in a subgroup of patients, spontaneous remission is encountered . In the remainder, which accounts for 60% of all affected individuals, even with treatment severe disability or death are encountered .
In patients who respond to treatment, imaging follow-up demonstrates regression of the aforementioned inflammatory findings.
Differential diagnosis
The diagnosis of inflammatory cerebral amyloid angiopathy on clinicoradiologic grounds requires the exclusion of other causes:
- infection, such as progressive multifocal leukoencephalopathy (PML) or meningoencephalitis of various causes
- vascular pathologies, such as primary CNS vasculitis or posterior reversible encephalopathy syndrome (PRES)
- neoplasm, such as metastases
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Inflammatory cerebral amyloid angiopathy:
Assoziationen und Differentialdiagnosen zu Inflammatory cerebral amyloid angiopathy: