intrakranielle Epidermoidzyste






































Intracranial epidermoid cysts are uncommon congenital lesions which account for about 1% of all intracranial tumors. They result from inclusion of ectodermal elements during neural tube closure, and typically present in middle age due to mass effect on adjacent structures. Their content, derived from desquamated epithelial cells, mimics CSF on CT and MRI, with the exception of DWI which demonstrates restricted diffusion. Management is surgical and prognosis is good.
Epidemiology
Although predominantly congenital, epidermoid cysts are usually very slow growing and as such take many years to present. Typically patients are between 20 and 40 years of age . There may be increased prevalence in males, although this is not found in all series .
Epidermoid cysts account for ~1% of all intracranial tumors .
An uncommon association exists with anorectal anomalies, sacral anomalies and presacral mass, and is known as the Currarino triad .
Clinical presentation
Signs and symptoms of epidermoid cysts are due to gradual mass effect, with presentation including :
- headaches: most common
- cranial nerve deficits
- cerebellar symptoms
- seizures
- raised intracranial pressure
Recurrent aseptic meningitis is uncommon but recognized, similar to the less common dermoid cyst .
Pathology
Epidermoid cysts may be congenital (most common, arising from ectodermal inclusion during neural tube closure ) or acquired (post-surgical or post-traumatic implantation). Pathologically, intracranial epidermoid cysts are identical to the petrous apex and middle ear congenital cholesteatomas. They differ from dermoid cysts which have both epidermal and skin appendages such as hair and sebaceous cysts and mature teratomas which have all three layers.
They have a thin capsule which is made of a thin layer of squamous epithelium, which macroscopically is white and pearly, and may be smooth, lobulated, or nodular. Internal cystic components are often filled with desquamated epithelial keratin and cholesterol crystals; grossly appearing as a creamy, waxy material. It should be noted that some authors contest that epidermoid cysts are along a spectrum which includes cystic (adamantinomatous) craniopharyngiomas, which have some histological similarities . Cholesterol and keratin components account for their distinct imaging characteristics .
Location
- intradural: 90%
- cerebellopontine angle: 40-50%
- third most common cerebellopontine angle mass, after acoustic schwannomas and meningiomas, and accounts for approximately 5-10% of all tumors in this region
- suprasellar cistern: 10-15%
- fourth ventricle: ~17%
- middle cranial fossa
- interhemispheric: < 5%
- spinal (rare)
- cerebellopontine angle: 40-50%
- extradural: 10%
- most within skull
Radiographic features
Intracranial epidermoid cysts appear as lobulated lesions that fill and expand CSF spaces and exert a gradual mass effect, insinuating between structures and encasing adjacent nerves and vessels. A common feature of posterior fossa cysts is displacement of the basilar artery away from the pons.
CT
The combination of cellular debris along with a high cholesterol content lower the density of epidermoids to approximately 0 HU, and can thus be identical in density to CSF, and look the same as an arachnoid cyst.
Calcification is seen in a minority of cases (10-25% ), and rarely an epidermoid cyst may be hyperdense due to hemorrhage, saponification or high protein content ("white epidermoids"). The interhemispheric epidermoids are reported to have peripheral calcification.
They do not enhance and only very rarely demonstrate any enhancement of the wall.
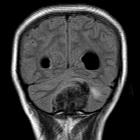
MRI
Similar to CT, epidermoids are often indistinguishable from arachnoid cysts or dilated CSF spaces on many MR sequences, except for DWI/ADC which helps to differentiate them.
- T1
- usually isointense to CSF
- higher signal compared to CSF around the periphery of the lesion is frequently seen
- rarely they can be of high signal and are known as white epidermoids
- rare intralesional hemorrhage can also result in intrinsic high signal
- T1 C+ (Gd)
- thin enhancement around the periphery may sometimes be seen
- in the rare cases of malignant degeneration, enhancement becomes more pronounced
- T2
- usually isointense to CSF (65%)
- slightly hyperintense (35%) to grey matter
- rarely hypointense to grey matter, usually in the setting of the so-called white epidermoid (the term refers to the T1 appearance)
- FLAIR
- often heterogeneous/dirty signal; higher than CSF
- beware of flow artefact from CSF pulsation which can mimic this appearance
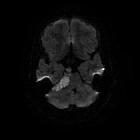
- DWI/ADC
- useful for differentiation from arachnoid cysts due to increased signal (due to a combination of abnormal restricted diffusion and T2 shine through), which is not seen with arachnoid cysts
Treatment and prognosis
Surgical excision is the treatment of choice if symptomatic. However, complete resection is difficult as not all tissue can be removed, especially from around cranial nerves and vessels. Recurrence is therefore not uncommon, although growth is typically slow and many years can elapse without new symptoms.
Differential diagnosis
The differential for an epidermoid cyst include:
- CSF collections, e.g. arachnoid cyst or mega cisterna magna
- less lobulated
- displaces vessels
- follows CSF on all sequences, including FLAIR and DWI
- dermoid cyst
- often fat density due to sebum
- typically located along the midline
- inflammatory cyst, e.g. neurocysticercosis
- smaller, but can be multiple
- may enhance peripherally
- may have associated edema
- usually no restricted diffusion
- cystic tumors, e.g. acoustic schwannoma or craniopharyngioma
- a solid enhancing component is usually identifiable
- neurenteric cyst
Siehe auch:
- Mega Cisterna magna
- Arachnoidalzyste
- Neurozystizerkose
- Pinealiszyste
- Dermoidzyste
- Kraniopharyngeom
- Tumoren der Pinealisregion
- epidermale Inklusionszyste
- Vestibularisschwannom
- spinale Epidermoidzyste
- neuroenterische Zyste
- intraventricular epidermoid
- Epidermoid
- Epidermoidzyste der Kalotte
und weiter:
- Epidermoidzyste
- white epidermoid
- intrakranielle Dermoidzyste
- Epidermoidzyste im Kleinhirnbrückenwinkel
- Epidermoidzyste vs Dermoidzyste
- diffusion MRI of an epidermoid tumor
- rupturierte intrakranielle Dermoidzyste
- Tumor vor der Medulla oblongata
- intrakranielle zystische Läsionen
- Epidermoidzyste der Glandula pinealis
- cystic lesion brain
- epidermoid cyst compressing the trigeminal nerve
- fetthaltiger Dermoidtumor
- suprasellar epidermoid tumor
- epidermoid tumor of the cerebellopontine angle
- congenital intracranial dermoid tumor
- epidermoid cyst pre-pontine


 Assoziationen und Differentialdiagnosen zu intrakranielle Epidermoidzyste:
Assoziationen und Differentialdiagnosen zu intrakranielle Epidermoidzyste:










