Lymphom des Magens



















Gastric lymphoma may either represent secondary involvement by systemic disease or primary malignancy confined to the stomach.
Epidemiology
Gastric lymphoma represents the most common site of extranodal lymphoma, accounting for 25% of all such lymphomas, 50% of all gastrointestinal lymphomas, but comprise only 1-5% of all gastric malignancies .
Typically primary gastric lymphoma occurs in adults in the 6 decade of life, without a distinct gender predilection . Secondary gastric lymphoma matches the demographics of the underlying lymphoma.
Clinical presentation
Typically patients present with long-standing epigastric pain and/or dyspepsia often attributed to Helicobacter pylori .
Pathology
Three distinct types of gastric lymphoma are recognized :
Mucosa-associated lymphoid tissue (MALT) lymphoma is strongly associated with Helicobacter pylori (85-98% of cases). These are low-grade lymphomas and may regress following the treatment of Helicobacter infection .
Radiographic features
Fluoroscopy
Appearances on barium meal vary from normal to grossly abnormal. Possible findings include:
- bull's eye appearance due to central ulceration
- filling defects
- thickened gastric rugae
- linitis plastica
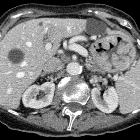
CT
Typically gastric lymphoma demonstrates marked thickening of the stomach wall (2-4 cm) with a large lateral extension of the tumor (i.e. along the wall of the stomach) representing submucosal spread .
In some instances the submucosal spread encompasses the majority of the stomach, giving it a linitis plastica appearance. Such extensive mural involvement can also extend across the pylorus into the duodenum and superiorly into the esophagus .
Despite such extensive involvement, it is uncommon for lymphoma to result in gastric outlet obstruction or perigastric fat invasion.
The mass is usually homogeneous in attenuation, but may contain focal areas of low density representing necrosis.
Extensive retroperitoneal and local nodal enlargement is often seen.
Differential diagnosis
General imaging differential considerations include:
- gastric carcinoma
- more likely to cause gastric outlet obstruction
- more likely to be in the distal stomach
- more likely to extend beyond the serosa and obliterate adjacent fat plane
- more focal
- lymph nodes tend to be smaller and more localized to immediate draining nodes (unlike in gastric carcinoma, gastric lymphomas are associated with large lymph nodes and with adenopathy often extending below the level of renal veins/hilum)
- gastrointestinal stromal tumor (GIST)
For diffuse gastric wall thickening also consider:
- gastritis
- Menetrier's disease: has a rugal like pattern
Siehe auch:
- verdickte Magenwand
- phlegmonöse Gastritis
- Adenokarzinom des Magens
- Gastrointestinaler Stromatumor
- Morbus Ménétrier
- Burkitt-Lymphom des Magens
und weiter:


 Assoziationen und Differentialdiagnosen zu Lymphom des Magens:
Assoziationen und Differentialdiagnosen zu Lymphom des Magens: