lymphoma vs toxoplasmosis
Toxoplasmosis and lymphoma are frequently differential diagnoses in patients with HIV/AIDS, as these represent the most common brain lesions with mass effect in this population. As treatment is substantially different, distinguishing the two on imaging is important, particularly when the lesion involves areas that are risky to biopsy.
In some instances, the imaging appearance is classic and differentiation is not problematic; however, in 50-80% of cases, the appearances can be very similar . Below are helpful distinguishing features.
For a general discussion on each diagnosis, please refer to the individual articles: cerebral toxoplasmosis and primary CNS lymphoma.
Radiographic features
Distribution
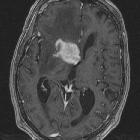
Primary CNS lymphoma typically demonstrates subependymal spread, whereas toxoplasmosis tends to be scattered through the basal ganglia and at the corticomedullary junction .
HIV lymphoma also is far more frequently a solitary lesion, whereas toxoplasmosis is usually multifocal (86%) .
Enhancement
On CT and MRI, both entities enhance following administration of contrast. Lymphoma may solidly enhance, whereas toxoplasmosis usually demonstrates ring or nodular enhancement .
However, in the setting of HIV/AIDS, primary CNS lymphoma may also demonstrate peripheral enhancement. Thus, the pattern of enhancement may not be helpful.
Hemorrhage
Hemorrhage is uncommon in lymphoma, especially prior to treatment, but may be seen occasionally in toxoplasmosis.
MR diffusion
Toxoplasmosis and lymphoma have significant overlap in terms of diffusion characteristics, but toxoplasmosis tends to have more facilitated diffusion while lymphoma tends to have more restricted diffusion in the core of the lesion. Case-control studies of rim-enhancing lesions larger than 1 cm have reported the following regarding the cores of these lesions on DWI :
- ADC >1.6 times that of contralateral normal white matter favors toxoplasmosis
- ADC <0.8-1.0 times contralateral white matter favors lymphoma
MR spectroscopy
- both entities demonstrate increased lactate and lipids, although this tends to be less marked in lymphoma
- lymphoma typically demonstrates marked increase in choline, whereas it is reduced in toxoplasmosis
- both lesions demonstrate decreased creatine and NAA; however, this finding is variable
Ideally, MR spectroscopy (MRS) should be performed with both long and short TE sequences .
MR perfusion
A decrease in cerebral blood volume (rCBV) centrally within lesions suggests toxoplasmosis, whereas it is increased in lymphoma . Case-control studies using contemporary DSC MR perfusion techniques have reported the following :
- rCBV >1.3-1.5 times that of contralateral normal white matter favors lymphoma or other neoplasms (such as glioma or metastasis)
- rCBV <1.3-1.5 times contralateral white matter favors toxoplasmosis or other infection (such as fungal or bacterial abscess)
However, rCBV is reduced in the perilesional edema of both lesions .
SPECT
Thallium 201 chloride SPECT demonstrates increased uptake in lymphoma because thallium serves as a potassium analog and is avidly taken up by hypermetabolic tumor cells . By contrast, thallium activity is decreased in toxoplasmosis because there is no cellular correlate .
Practical points
Features that favor primary CNS lymphoma include:
- single lesion
- subependymal spread
- solid enhancement
- no hemorrhage before treatment
- thallium SPECT positive
- DWI: restricted diffusion
- MRS: increased choline
- MR perfusion: increased rCBV
Features that favor cerebral toxoplasmosis include:
- multiple lesions
- scattered throughout the basal ganglia and corticomedullary junction
- ring or nodular enhancement
- hemorrhage occasionally occurs mostly in the periphery of the lesion
- thallium SPECT negative
- DWI: facilitated diffusion
- MRS: decreased choline (Cho)
- MR perfusion: decreased rCBV
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu lymphoma vs toxoplasmosis:
Assoziationen und Differentialdiagnosen zu lymphoma vs toxoplasmosis: