Neurotoxoplasmose




























Neurotoxoplasmosis, also known as cerebral toxoplasmosis, is an opportunistic infection caused by the parasite Toxoplasma gondii. It typically affects patients with HIV/AIDS and is the most common cause of cerebral abscess in these patients .
Congenital toxoplasmosis, as well as congenital cerebral toxoplasmosis, are discussed separately.
Epidemiology
Toxoplasma gondii is found ubiquitously and antibodies to the organism can be identified in 30% of all humans. The rate varies greatly from population to population and has a wide reported prevalence: from 6-90% . In most cases, the infection is asymptomatic. However, in immunocompromised patients (especially those with HIV/AIDS), infection can become established. Cerebral toxoplasmosis is found in 10-34% of autopsies on patients with HIV/AIDS .
The infection most likely occurs once the CD4+ count has dropped below 200 cells/mm .
Clinical presentation
In immunocompetent patients, acute encephalitis is extremely rare. Even in the immunocompromised, symptoms are typically vague and indolent. Development of new neurological symptoms in these patients should raise high suspicion of cerebral toxoplasmosis.
Pathology
Toxoplasma gondii is an intracellular parasite that infects birds and mammals. Its definitive host is the cat and other Felidae species. Excretion of oocytes in its feces followed by contaminated uncooked consumption by humans can lead to human infection. In immunocompetent individuals, it primarily causes a subclinical or asymptomatic infection. In immunocompromised individuals (e.g. AIDS patients), toxoplasmosis is the most common cause of a brain abscess.
Pathologically, parenchymal toxoplasma lesions have three distinct zones:
- a central avascular zone of coagulative necrosis
- an intermediate vascular zone containing numerous organisms
- an outermost zone of encysted organisms; Toxoplasma lesions do not have a capsule
Radiographic features
Typically cerebral toxoplasmosis manifest as multiple lesions, with a predilection for the basal ganglia, thalami, and corticomedullary junction .
CT
Typically, cerebral toxoplasmosis appears as multiple hypodense regions predominantly in the basal ganglia and at the corticomedullary junction. However, they may be seen in the posterior fossa. Size is variable, from less than 1 cm to more than 3 cm, and there may be associated mass effect.
- enhancement: following administration of contrast there is nodular or ring enhancement which is typically thin and smooth
- double-dose delayed scan: may show a central filling on delayed scans
- calcification: seen in treated cases; may be dot-like or thick and 'chunky'
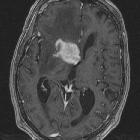
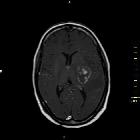
MRI
- T1: may be difficult to identify, but are typically isointense or hypointense
- T2
- intensity is variable, from hyperintense to isointense
- hyperintense: thought to represent necrotizing encephalitis
- isointense: thought to represent organizing abscess
- concentric alternating zone of hypo/hyper/isointense signal
- also known as 'concentric target sign'
- lesions are surrounded by perilesional edema
- intensity is variable, from hyperintense to isointense
- T1 C+ (Gd): lesions often demonstrate ring enhancement or nodular enhancement. For this pathology is also typically еccentric target sign on post-contrast images
- MR spectroscopy
- increased lactate
- increased lipids
- reduced Cho, Cr and NAA
- increased lipid-lactate peak is characteristic, however, choline peak also may be seen in few cases
PET/CT scan and thallium SPECT
Minimal or no uptake (cold lesion) as opposed to primary CNS lymphoma .
Treatment and prognosis
In general, biopsy is not required and treatment is initiated and follow-up imaging performed. The exception to this rule are patients who have atypical imaging features (e.g. single lesion) or who are seronegative for Toxoplasma gondii .
Treatment consists of sulfadiazine with pyrimethamine .
Differential diagnosis
General imaging differential considerations include:
- primary CNS lymphoma: see lymphoma vs toxoplasmosis
- cerebral metastases
- other infections
Siehe auch:
- Hirnmetastase
- Hirnabszess
- Neurozystizerkose
- Abszess
- primäres ZNS-Lymphom
- zerebrale Kryptokokkose
- fetal toxoplasmosis
- Toxoplasmose
- lymphoma vs toxoplasmosis
- Läsionen mit ringförmiger Kontrastmittelanreicherung
und weiter:
- zerebrale Verkalkungen
- intrakranielle Verkalkungen
- Glioblastoma multiforme
- Basalganglienverkalkungen
- butterfly glioma
- Tuberkulose des ZNS
- Brain stone
- neuroradiologisches Curriculum
- white matter changes in HIV
- Tuberkulom des ZNS
- pädiatrische zerebrale Infektionen
- acute necrotising toxoplasma encephalitis
- kongenitale zerebrale Toxoplasmose


 Assoziationen und Differentialdiagnosen zu Neurotoxoplasmose:
Assoziationen und Differentialdiagnosen zu Neurotoxoplasmose: