Abszess





















Abscesses are focal confined collections of suppurative inflammatory material and can be thought of as having three components :
Terminology
Abscesses are akin to empyemas, as both are defined inflammatory collections. The difference is that abscesses occur in the parenchyma of the affected organ while empyemas arise in a pre-existing cavity such as the pleural space.
Clinical presentation
The presentation of an abscess is varied depending on the location and its infiltration and mass effect on local structures. Systemically, patients with abscesses can present with swinging pyrexia and raised inflammatory markers, which are resistant to antimicrobial therapy. Pain is a common accompanying symptom. The hallmark signs of subcutaneous abscesses are pain, warmth, redness, and swelling.
Pathology
Etiology
Abscesses can be caused by bacteria, parasites, or fungi.
Location
Essentially any tissue in the body can play host to abscesses. Please refer to individual articles for further details:
- Bezold abscess
- breast abscess
- Brodie abscess
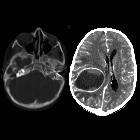
- cerebral abscess
- liver abscess
- pulmonary abscess
- renal abscess
- spinal epidural abscess
- splenic abscess
- subcutaneous abscess
Radiographic features
Typical radiological appearances are of a central zone of necrotic inflammatory material encapsulated by a discernible wall. Exact features will vary depending on the tissue or organ within which the abscess is located.
CT
- relatively low-attenuation central necrotic component
- a well-defined fibrous capsule: can be irregular and thick when compared to the thin smooth wall of a simple cyst
- capsular ring enhancement with contrast: can be difficult to appreciate when the abscess is contained in a vascular structure like the liver where there is a concurrent parenchymal enhancement
- surrounding inflammatory changes (i.e. peritoneal fat stranding)
- a mass effect with effacement of adjacent structures
Nuclear medicine
The presence of an abscess in patients presenting with sepsis can be delineated by indium (In-111) labeled white cell scans, often in the setting of suspected abdominopelvic sepsis. Tracer accumulates in the region of the abscess, such as the right iliac fossa in an appendiceal abscess.
As abscesses usually have a thick wall with poor vascularity, indium-111 take-up can be a lengthy process and 48-hour delayed images are sometimes required. The sensitivity of this test is not thought to be affected by the use of concomitant antibiotics or steroids.
Treatment and prognosis
Treatment is guided by the size, accessibility, and clinical severity of sepsis in each case. Although abscesses may be treated medically with antibiotics, they often require percutaneous or surgical drainage. As abscesses have poor vascularity, high dose oral or parenteral treatment is preferred. Percutaneous drainage can be performed under ultrasound or CT guidance for abscesses within the thoracic or peritoneal cavity. Some abscesses will require open incision and drainage.
History and etymology
The abscess is derived from the Greek work aposteme (άπό-ίστημι) meaning "throwing off of bad humors". The word first appeared in 1543 in a translation of a surgery text: "Aposteme - In latyne, it is called abscissas" .
Siehe auch:
- Hirnabszess
- Leberabszess
- Brodie-Abszess
- Lungenabszess
- Tuboovarialabszess
- Appendizitis mit Abszess
- Bezoldscher Senkungsabszess
- bakterieller Hirnabszess
und weiter:


 Assoziationen und Differentialdiagnosen zu Abszess:
Assoziationen und Differentialdiagnosen zu Abszess: