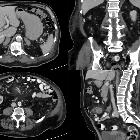
Malignes Melanom Metastase



















Metastatic melanoma is known for its aggressive nature and for its ability to metastasize to a variety of atypical locations, which is why it demonstrates poor prognostic characteristics.
Epidemiology
Melanoma accounts for ~5% of all skin cancers, however, it remains the leading cause of death amongst skin cancers. The risk of metastatic progression has a strong association with the site of the initial primary melanoma, with melanomas arising from the head, neck and trunk carrying a higher risk of metastatic progression than those melanomas arising from the limbs .
Pathology
The initial clinical staging of the primary malignant melanoma is essential and incorporates clinical and/or radiological evaluation for metastatic disease. The Breslow thickness and Clarke level of cutaneous melanoma classification has been widely discussed, as has the TNM staging protocol.
The most frequent site of involvement of metastatic disease is the lymphatic system, in particular the local and regional lymph nodes surrounding the primary melanoma. Further lymph node involvement typically progresses in a contiguous fashion .
The detection of melanoma spread to the lymph nodes is the most important predictor of survival and eventual disease recurrence with poor survival outcomes associated with sentinel lymph node involvement even after the initial removal of the sentinel lymph node and the surrounding nodal basin .
Radiographic features
Radiological assessment plays a vital role in both the initial diagnosis of metastatic melanoma and in assessing disease progression and treatment efficacy.
Nodal metastases
Metastatic spread to the lymph nodes represents the most common site of malignant melanoma metastases.
Ultrasound
- lymph nodes with metastatic disease may have an irregular, hypoechoic or lobulated appearance
CT
- imaging modality of choice to assess for nodal metastases
- increased regional nodal size and nodal heterogeneity have implications for metastatic disease
Thoracic metastases
The lungs and pleura are the second most common site of malignant melanoma metastases after lymph node involvement, with 85% of end-stage melanoma patients having evidence of lung metastases at autopsy .
PET-CT
- when combined with dedicated CT interpretation this remains the most sensitive imaging modality to characterize the extent of thoracic melanoma metastases
- pulmonary metastases are most commonly multiple rounded and sharply delineated lesions
- may less frequently present as a solitary pulmonary nodule
- mediastinal and hilar nodal involvement are common
CNS and head/neck metastases
Metastatic melanoma remains the third most common cause of intracranial metastases, behind both lung and breast cancer .
MRI
Imaging modality of choice for the interpretation of intracerebral metastases, demonstrating improved sensitivity and specificity when compared to contrast-enhanced CT .
Metastatic intracerebral lesions are most frequently seen involving the cortex and are then seen less frequently to involve the grey/white matter junction, the dura and the leptomeninges .
- T1: typically hyperintense due to a reduction in T1 relaxation time associated with the presence of melanin
- T2: reduced T2 signal
- T1 C+ (Gd): demonstrates peripheral rim enhancement with a heterogeneous pattern of enhancement
Abdominal and pelvic metastases
Melanoma metastases to the liver are the most common metastases involving the abdomen and pelvis and have been found in approximately 60-70% of melanoma patients at the time of autopsy .
CT
- single or multiple hepatic metastatic lesions which may be hypervascular on the arterial phase and hypodense on the portal venous phase
- rim enhancement with central necrotic features is commonly seen
- hepatic melanoma metastases often demonstrate low attenuation when compared to normal hepatic parenchyma on CT
MRI
Findings are similar to those previously described for intracranial metastatic melanoma:
- T1:
- hyperintensity secondary to the melanin content of melanocytes
- care must be taken when diagnosing these lesions as other lesions can also demonstrate T1W hyperintensity due to associated hemorrhage
PET-CT
When combined with dedicated CT, it a sensitivity of 98% and a specificity of 94% for detecting metastatic melanoma . Sites of metastases are normally FDG avid.
Skeletal metastases
appear as lytic lesions most commonly involving the axial skeleton
Treatment and prognosis
Treatment of metastatic melanoma is complex and depends entirely upon the extent and site of pathological disease involvement. Wide excision of the identified primary tumor is the initial treatment of choice, however, if regional node involvement is suspected then lymphadenectomy can be performed.
A combination of regional/systemic chemotherapy with associated immunotherapy and/or radiation therapy can be employed depending upon the individual clinical context.
Metastatic melanoma has a poor prognosis due to its aggressive nature and survival rates depend upon the staging of the disease. Patients with a single regional lymph node involvement have a 5-year survival rate of 80%, which then decreases depending upon the number of regional nodes involved. Individuals with evidence of distal disease have a poor prognosis with 5-year survival estimates being 22% for distal nodal involvement and fall to 8% for patients with other identified visceral metastatic disease .
Differential diagnosis
General imaging differential considerations include:
- other hypervascular metastatic disease
- lymphoma
- leukemia
- Kaposi sarcoma
- primary gastrointestinal tract malignancies
Siehe auch:
- Lebermetastasen malignes Melanom
- Malignes Melanom
- Hirnmetastasen Malignes Melanom
- Malignes Melanom Dünndarmmetastasen
- melanocytic lesions of the central nervous system
- Melanommetastasen im Thymus
- Metastasen bei Aderhautmelanom
- Knochenmetastasen malignes Melanom
- Malignes Melanom Lungenmetastasen
und weiter:


 Assoziationen und Differentialdiagnosen zu Malignes Melanom Metastase:
Assoziationen und Differentialdiagnosen zu Malignes Melanom Metastase:



