mesial temporal sclerosis (MTS)

























Mesial temporal sclerosis (MTS), also commonly referred to as hippocampal sclerosis, is the most common association with intractable temporal lobe epilepsy (TLE) . It is seen in up to 65% of autopsy studies, although significantly less on imaging.
Clinical presentation
Most patients present with complex partial temporal lobe epilepsy.
Febrile seizures
The relationship, if any, of mesial temporal sclerosis with febrile seizures is controversial, made all the more difficult due to the relative insensitivity of imaging and the difficulty in establishing whether a particular seizure was truly febrile. Up to a third of patients with established refractory temporal lobe epilepsy have a history of seizures in childhood at the time of fever . Follow up of children with febrile seizures does not demonstrate significant increased incidence of temporal lobe epilepsy .
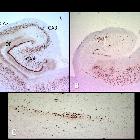
Pathology
The hippocampal formation is not uniformly affected, with the dentate gyrus, and the CA1, CA4 and to a lesser degree CA3 sections of the hippocampus being primarily involved . Histologically there is neuronal cell loss, gliosis and sclerosis.
Etiology
Controversy exists as to the causative mechanism: is mesial temporal sclerosis a result of temporal lobe epilepsy or vice versa ? In children with newly diagnosed epilepsy, only ~ 1% have evidence of MTS on imaging . Furthermore, in adults 3-10% of cases of mesial temporal sclerosis demonstrate bilateral changes even though symptoms may be unilateral.
Radiographic features
MRI
MRI is the modality of choice to evaluate the hippocampus, however dedicated TLE protocol needs to be performed if good sensitivity and specificity is to be achieved . Thin section angled coronal sequences at right angles to the longitudinal axis of the hippocampus are required, to minimize volume averaging.
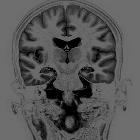
Coronal volume and coronal high resolution T2WI/FLAIR are best to diagnose MTS.
Findings include :
- reduced hippocampal volume: hippocampal atrophy
- increased T2 signal
- abnormal morphology: loss of internal architecture (interdigitations of hippocampus), stratum radiata, a thin layer of white matter separates the dentate nucleus and Ammon horn
Although comparing left to right side is easiest, it must be remembered that up to 10% of cases are bilateral, and thus if symmetry is the only feature being evaluated, many cases may be misinterpreted as normal.
Often mentioned, but probably one of the least specific findings, is enlargement of the temporal horn of the lateral ventricle . If anything, care must be taken not to allow an enlarged horn to trick you into thinking the hippocampus is reduced in size.
When severe and long standing, additional associated findings include :
- atrophy of the ipsilateral fornix and mammillary body
- increased signal and or atrophy of the anterior thalamic nucleus
- atrophy of the cingulate gyrus
- increased signal and/or reduction in the volume of the amygdala
- reduction in the volume of the subiculum
- dilatation of temporal horn and temporal lobe atrophy
- collateral white matter and entorhinal cortex atrophy
- thalamic and caudate atrophy
- ipsilateral cerebral hypertrophy
- contralateral cerebellar hemiatrophy
- loss of grey-white matter interface in the anterior temporal lobe
- reduced white matter volume in the parahippocampal gyrus
Additional 3D volumetric studies can be performed, and although time consuming to post-process may be more sensitive to subtle hippocampal volume loss. Gadolinium is not required .
T2 relaxometry may also be useful in detecting cases of hippocampal sclerosis .
Diffusion MRI
As a result of neuronal loss, the extracellular space is enlarged and thus diffusion of water molecules is greater on the affected side, resulting in increased values on the affected side (higher signal on ADC).
Conversely, due to neuronal dysfunction and swelling, diffusion is restricted following a seizure, and thus values are lower .
MR spectroscopy
MR spectroscopy findings typically represent neuronal dysfunction :
- decreased NAA and decreased NAA/Cho and NAA/Cr ratios
- decreased MI in ipsilateral temporal lobe
- increased lipid and lactate soon after as seizure
MR perfusion
MR perfusion demonstrates similar changes to SPECT (see below) with blood perfusion depending on when the scan is obtained.
During the peri-ictal phases, perfusion is increased, not only in the mesial temporal lobe but often in large parts of temporal lobe and hemisphere. In interictal periods, conversely, perfusion is reduced .
Nuclear medicine
SPECT (Tc-99m HMPAO or ECD) and PET (F18-FDG) imaging are also a useful adjuncts, with both ictal and interictal scans demonstrating abnormalities:
- ictal scan: hyperperfusion
- interictal scan: hypoperfusion
Other causes of temporal lobe epilepsy (TLE) should be considered, especially as small temporal lobe cortical tumors can have similar appearances.
Treatment and prognosis
TLE is initially managed medically with anti-epileptic agents. In patients who are refractory to medical management temporal lobectomy or selective amygdalohippocampectomy may be performed. Anterior temporal lobectomy is successful in 75-90% of patients with MTS.
Siehe auch:
und weiter:


 Assoziationen und Differentialdiagnosen zu Hippocampussklerose:
Assoziationen und Differentialdiagnosen zu Hippocampussklerose:
