Metastasen der Schädelbasis

Metastasen der Schädelbasis
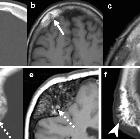
Knochenmetastasen des Schädels Radiopaedia • CC-by-nc-sa 3.0 • de
Metastases to the skull are very common in patients with disseminated skeletal metastatic disease, although they are often asymptomatic. For a more detailed general discussion please refer to the article on skeletal metastatic disease.
Epidemiology
Skull metastases are seen in ~20% (range 15-25%) of all cancer patients . The demographics of patients with skull metastases will mirror those of the primary tumor, and as such in general they are found in the older population.
Clinical presentation
Although over half of all skeletal metastases are asymptomatic, they can cause symptoms in a number of scenarios :
- mass effect on adjacent structures
- mechanical instability
- occipital condyle compression fracture
- temporomandibular joint instability
Pathology
Primary tumors most frequently encountered as metastases to the skull include :
- breast cancer
- lung cancer
- melanoma
- prostate cancer
- thyroid cancer (usually follicular)
- renal cell cancer
- lymphoma
- leukemia
- multiple myeloma
- intrahepatic cholangiocarcinoma
In children both neuroblastoma (skull metastases are not infrequently the first sign of disease) and Ewing sarcoma are encountered.
Radiographic features
Skull metastases have the same range of appearances as skeletal metastases elsewhere, and in 90% of cases other skeletal metastases are evident:
- lytic metastases: most common
- sclerotic metastases
- can particularly occur from breast and prostate cancers
- mixed lytic and sclerotic metastases
It is worth remembering that occasionally a solitary skull metastasis may be the only evidence of metastatic disease. This is particularly the case with renal cell carcinoma and thyroid carcinoma .
Treatment and prognosis
For asymptomatic lesions, no specific treatment is required above or beyond systemic treatment being administered. Even when symptomatic, in many instances patients are being palliated and as such no focal therapy is instituted.
In instances where symptoms are significant and the general health and prognosis warrants intervention, a number of options exist :
- radiotherapy
- whole brain radiotherapy if cerebral or leptomeningeal metastases are present
- focal radiotherapy for single/symptomatic lesions
- chemotherapy
- usually already instituted for systemic disease
- surgery
- reserved for larger symptomatic lesions
- has a role in diagnosis, when the lesion is solitary or diagnosis not established
It is difficult to say anything sensible when discussing prognosis, as clearly the degree of systemic disease, and the primary tumor and its response to therapy is going to have a huge impact. In general, it is safe to say however that in most instances, skeletal metastases represent advanced disease with poor prognosis, typically measured in weeks and months.
Siehe auch:


 Assoziationen und Differentialdiagnosen zu Metastasen der Schädelbasis:
Assoziationen und Differentialdiagnosen zu Metastasen der Schädelbasis: