Osteolysen der Kalotte
Imaging of
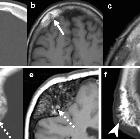
skull vault tumors in adults. Bone hemangiomas. Case 1 (a–c): CT (a), T1WI (b), and T2WI (c) show well-defined lytic lesion, with thickened cortical and medullar trabecular spaces (arrows in a), and internal T1 and T2 hyperintense signal corresponding to fat and vascular tissue (arrows in b and c). Case 2 (d, e): CT (d) and T1WI (e) show marked bone expansion, fat content (dashed arrows), and strikingly enlarged trabecula producing a “spoke-wheel” appearance. Case 3 (f): CT depicts interruption of outer cortical table with overcoming enlarged spiculated trabecula simulating aggressive periosteal reaction (arrowhead)

Imaging of
skull vault tumors in adults. Hemangiopericytoma. CT (a), T2WI (b), and post-contrast T1WI (c). Dural-based “mushroom-like” mass (arrows) with brain edema (dashed-arrows), intense homogeneous enhancement, and foci of bone lysis (arrowhead)

Osteoma •
Mastoid osteoma - Ganzer Fall bei Radiopaedia
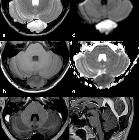
Eosinophiles
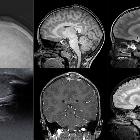
Granulom der Schädelkalotte. Oben konventionelles Röntgen, MRT sagittal T1 und T2; unten Sonografie MRT koronar T1 und sagittal FLAIR.

Lytic skull
lesion • Multiple myeloma - Ganzer Fall bei Radiopaedia

Spectrum of
lytic lesions of the skull: a pictorial essay. Intradiploic epidermoid cyst (IEC). Axial CT images with soft tissues (a) and bone (b) windows show an occipital hypodense osteolytic lesion with smooth margins and greater involvement of the inner table, extensively demineralised

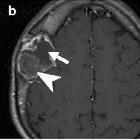
Intradiploic
epidermoid cyst with osteolytic lesions of the skull.. Axial post gadolinium T1-weighted MR images show minimal and peripheral contrast enhancement (arrows).

Intradiploic
epidermoid cyst with osteolytic lesions of the skull.. Axial FLAIR images demonstrate an inhomogeneous hyperintense lesion in the right occipital intradiploic space (arrows).

Intradiploic
epidermoid cyst with osteolytic lesions of the skull.. Axial T2-weighted images demonstrate an inhomogeneous hyperintense lesion in the right occipital intradiploic space (arrows).

Intradiploic
epidermoid cyst with osteolytic lesions of the skull.. Computed tomography scan with bone density window reveal an occipital osteolytic lesion (arrows).

Imaging of
skull vault tumors in adults. Osteomas. Multiple in Gardner syndrome. NECT show mass-like proliferation of normal appearing cortical bone in the frontal (arrow) and cortical and medullary bones in the parieto-occipital (dashed arrow) lesions

Langerhans
cell histiocytosis (skeletal manifestations) • Langerhans cell histiocytosis - Ganzer Fall bei Radiopaedia

Spectrum of
lytic lesions of the skull: a pictorial essay. Arachnoid granulations (AGs). Axial computed tomography (CT) images with brain (a) and bone (b) windows showing two well-defined, round-shaped lesions with cerebrospinal fluid (CSF) density, protruding into the calvarium along the right transverse sinus
Spectrum of
lytic lesions of the skull: a pictorial essay. Venous lacuna (VL). Axial CT image with bone (a) window showing a lytic lesion within the left parasagittal diploic space (arrowhead), confirmed on T2-weighted sequence (b). In a caudal slice, a right parasagittal AG can be depicted (c, d)

Spectrum of
lytic lesions of the skull: a pictorial essay. Intraosseous haemangioma (IH). Coronal (a) and axial (b) reformats of a CT scan with bone window indicate a left frontal expansive lesion with thin margins and intralesional spicules, radiating from a common centre, which erodes the outer layer of the skull, with relative sparing of the inner table
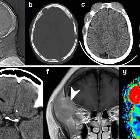
Spectrum of
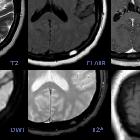
lytic lesions of the skull: a pictorial essay. IEC. On MR images of the same patient shown in Fig. 3, the lesion appears slightly inhomogeneous, mostly hyperintense on T2w (a) and hypointense on T1w (b) images, without contrast enhancement (c), showing diffusion restriction on b 1000 diffusion-weighted imaging (DWI) and the apparent diffusion coefficient (ADC) map (d, e). It causes compression on the confluence of sinuses (sagittal contrast-enhanced T1w image, f). As a consequence, the patient presented with intracranial hypertension symptoms
Imaging of
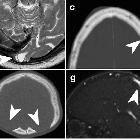
skull vault tumors in adults. Myeloma and plasmacytoma. Upper row. Myeloma. X-ray (a) NECT (b, c) and T1WI (d). Multiple “punched-out” lytic lesions with variable soft tissue components (a–c). Mandibular lesion suggesting myeloma instead of metastases (arrow in d). Note also the clival lesion (dashed arrow in d). Lower row. Plasmacytoma. NECT (e), T1WI post-contrast (f), and DSC-PWI (g). Single purely lytic transdiploic lesion with narrow zone of transition (arrows in e), hyperdense, hyperenhancing, and hypervascular (arrowheads respectively in e–g)

Spectrum of
lytic lesions of the skull: a pictorial essay. Aneurysmal bone cyst (ABC). Axial CT images with brain (a) and bone (b) windows show a left frontal lytic lesion with blood-fluid levels, associated with a diffuse ground-glass modification of the frontal bone, related to the presence of a fibrous dysplasia. Magnetic resonance (MR) examination better depicts the multiloculated lesion, confirming blood-fluid levels on T1w (c), FLAIR (d) and DWI (e) images, and showing enhancement of the capsule and internal septa (f)

Spectrum of
lytic lesions of the skull: a pictorial essay. Bone desmoplastic fibroma (DF). Axial CT images with soft tissues (a) and bone (b) windows showing a right parietal lytic lesion without erosion of the inner and outer tables

Spectrum of
lytic lesions of the skull: a pictorial essay. DF, same patient shown in Fig. 7. On MRI, the lesion presents a typical low signal intensity on T2w and T1w sequences (a, c), without diffusion restriction on the ADC map (b) or enhancement after contrast administration (d)

Spectrum of
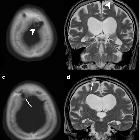
lytic lesions of the skull: a pictorial essay. Eosinophilic granuloma (EG). Axial CT images with soft tissues (a) and bone (b) windows showing a right frontal lytic lesion with ill-defined margins extending in the contiguous extracranial soft tissues. Erosion of the inner cranial table is more pronounced than of the outer (“hole within a hole” sign). 18(F) FDG-PET CT examination demonstrates a moderate tracer uptake (c, d)

Spectrum of
lytic lesions of the skull: a pictorial essay. EG, same patient shown in Fig. 9. On T1w (a) and T2w (b) images, the lesion appears mildly inhomogeneous, with diffusion restriction on the ADC map (c). MRI allows for an accurate evaluation of the surrounding soft tissues, as well as intracranial extension after contrast administration (d), causing a moderate dural thickening

Spectrum of
lytic lesions of the skull: a pictorial essay. Primary lymphoma of the bone. Axial CT images with soft tissues (a) and bone (b) windows highlight the presence of a bone lesion of the squamous portion of the left temporal bone, with lytic permeative pattern, extending to temporal extracranial soft tissues

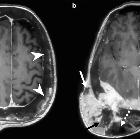
Spectrum of
lytic lesions of the skull: a pictorial essay. Primary lymphoma of the bone, same patient shown in Fig. 11. On MRI, the lesion demonstrates low T2 signal on axial (a) and coronal (b) T2-weighted sequences and extension to the temporal fossa and to the epidural space of the middle cranial fossa. The tumour exhibits homogeneous contrast enhancement; axial T1-weighted before (c) and after (d) contrast administration

Spectrum of
lytic lesions of the skull: a pictorial essay. Multiple myeloma (MM). Axial CT images with bone window showing multiple osteolytic lesions varying in shape and size, involving the skull vault and base

Intradiploic
epidermoid cyst with osteolytic lesions of the skull.. The ADC maps reveal restricted diffusion (arrows).
Imaging of
skull vault tumors in adults. Fibrous dysplasia. T2WI (a), post-contrast T1WI (b), and NECT (c). Expansile lesion with distinct lytic-cystic component (arrows) and “ground-glass” fibrous tissue (arrowheads) clearly depicted on NECT, deeply T2-hypointense, which enhances heterogeneously
Imaging of
skull vault tumors in adults. Osteosarcoma. Secondary, “pagetic.” T1WI post-contrast (a and b). Aggressive, destructive, giant, and transdiploic lesion with extensive intra- and extracranial soft-tissue component containing iso to hypointense areas of probable necrosis (arrows in a and b) and deeply hypointense foci of suspected bone matrix (dashed arrows in b). Note the underlying abnormal calvarial bone with diffuse expansion, cortical thickening and heterogeneous multifocal variable signal intensity, and enhancement (arrowheads) consistent with Paget disease

Osteoma •
Skull osteoma - Ganzer Fall bei Radiopaedia

Lytic skull
lesion • Luckenschadel skull - Ganzer Fall bei Radiopaedia

Lytic skull
lesion • Intradiploic epidermoid cyst - Ganzer Fall bei Radiopaedia

Lytic skull
lesion • Langerhans cell histiocytosis - Ganzer Fall bei Radiopaedia

Mammakarzinom
mit osteolytischen Metastasen: Computertomographie des Schädels axial Knochenfenster. Zu sehen ist eine größere Osteolyse frontal und mehrere kleinere.

Imaging of
skull vault tumors in adults. Metastases. Lytic metastases (a–f). CT of three patients (a–c) shows: a Solitary with narrow zone of transition (arrows), b multiple with slight soft-tissue components, and (c) solitary, giant, with mixed necrotic (arrowhead) and hypervascular (dashed arrows) soft tissue. Another case (d–f) with T2WI, T1WI post-contrast, and DSC-PWI shows solitary, giant, solid-enhancing, and hypervascular soft-tissue component (arrowheads). g–i Three cases of blastic metastases. Multiple (g). Aggressive periosteal reaction (arrows in h–i)

Osteoma •
Giant skull vault osteoma involving orbital roof - Ganzer Fall bei Radiopaedia

Osteoma •
Calvarial osteoma - Ganzer Fall bei Radiopaedia

Osteoma •
Skull osteoma - Ganzer Fall bei Radiopaedia

Osteoma •
Skull osteoma - Ganzer Fall bei Radiopaedia

Radiological
review of skull lesions. Osseous venous vascular malformation. Sagittal T1-weighted imaging (a), axial T2-weighted imaging (b) and sagittal contrast-enhanced venogram (c) show a hypointense T1, hyperintense T2 and enhancing lesion in the occipital bone (arrows)
Imaging of
skull vault tumors in adults. Calvarial pseudolesions. NECT (a, c–f), T2WI (b), MR venography (g, h). Parasagittal occipital arachnoid granulation (a). Occipital encephalocele (b). Dilated vascular canals and lacunae (c). Hyperostosis frontalis interna (d). Bilateral thinning of the parietal bones (e). Enlarged parietal foramina (f). Congenital sinus pericranii (g). Iatrogenic acquired sinus pericranii from a prior ventricular drainage (h)

Radiological
review of skull lesions. Langerhans cell histiocytosis. Sagittal skull radiograph (a) shows two lytic lesions (arrowheads) in the parietal skull, the largest one with an associated soft tissue component (thin arrow). Axial head CT images (b, c) in the bone and soft tissue windows in the same patient demonstrate an osseous destructive lesion in the left frontal calvarium with bevelled edges (dashed arrows) and a soft tissue component (thick arrows); pathology proven eosinophilic granuloma in a 4-year-old boy

Imaging of
skull vault tumors in adults. Lymphoma. Case 1 (a–d): NECT (a, b), post-contrast T1WI (c), and ADC map (d). Transdiploic mass with bone subtle sclerosis (arrows) and disproportionate soft-tissue components dense on CT, homogenously enhancing, and diffusion-restricting (arrowheads). Case 2 (e–g): Similar findings with bone lytic-permeation (arrows) instead

Imaging of
skull vault tumors in adults. Meningioma. Great polymorphism. Case 1 (a, b): Post-contrast T1WI (a) and CT (b): dural-based with dural tails (arrows) and bone lysis (dashed arrows). Case 2 (c–e): Post-contrast T1WI (c), CT (d), and DSC-PWI (e): dural-based hypervascular (arrowhead) with transdiploic growing (arrows), bone sclerosis-permeation, and aggressive-like periosteal reaction (dashed arrows). Case 3 (f, g): Post-contrast T1WI (f) and CT (g): diploic-centered plaque-like with intra- and extracranial laminar soft-tissue (arrowheads) and bone lysis-permeation (arrows). Case 4 (h): CT shows diploic-centered lesion with great spiculated hyperostosis (arrows). Case 5 (i, j) Post-contrast T1WI (i) and MR venography (j): diploic-centered with great homogeneous smooth hyperostosis (arrowhead) and intracranial soft-tissues characteristically invading the superior longitudinal venous sinus (arrows)

Imaging of
skull vault tumors in adults. Giant cell tumor of the bone. Axial NECT (a), T2WI (b), and T1WI post-contrast (c). Purely lytic lesion with severe expansion and cortical thinning (arrowhead in a), markedly T2 hypointense tissue content (arrow in b), and avid contrast-enhancement (dashed arrow in c)

Multisystemic
Langerhans cell hystiocitosis - Head and neck involvement. Well-defined lytic lesion with a double contour (hole within a hole = button sequestrum) and geographic margins, associated to a growing soft-tissue mass (yellow arrows). Prat-Matifoll J.A, Radiology Department, Vall Hebron Hospital

Imaging of
skull vault tumors in adults. Aneurysmal bone cyst (ABC). Case 1 (a–c): Primary ABC: NECT (a), T2WI (b), and post-contrast T1WI (c) show an extremely expansile, lytic, multiloculated, septated lesion, with severe cortical thinning (arrowhead in a), fluid-fluid levels (dashed arrow in b), and lineal enhancement (arrows in c). Case 2 (d–f): Fibrous dysplasia with secondary ABC: NECT demonstrates an expansile, lytic lesion with severe cortical thinning (arrowhead in d), a characteristic fluid-fluid level (arrow in f), and associated areas of “ground-glass” matrix (dashed arrows in e)

Imaging of
skull vault tumors in adults. Eosinophilic granuloma. NECT depicts inner and outer table endosteal scalloping and erosions (arrows in a) and bone sequestra (arrowhead in b). On T2WI (c), the lesion is hyperintense and bone sequestra could also be suspected (arrowhead). T1WI post-contrast (d) demonstrates intense enhancement and cranio-caudal orientation (dashed arrow)

Imaging of
skull vault tumors in adults. Epidermoid cysts (a–c and d–f) and dermoid cyst (g–i). Case 1 (a–c): Extracranial soft-tissue mass (arrows) remodeling the outer table on NECT (a), with fluid T2-signal (b), and markedly restricted diffusion (b = 1000) (c). Case 2 (d–f): Transdiploic mass (arrowheads), predominantly intracranial, T1WI (d) and T2WI (e) heterogenous and intense diffusion restriction (f). Case 3 (g–i). Frontal skull lesion (dashed arrows) disrupting the inner table on CT (g, h); content is CT-hypodense and T1-hyperintense, corresponding to fat (i)

Lytic skull
lesion • Eosinophilic granuloma - Ganzer Fall bei Radiopaedia

Spectrum of
lytic lesions of the skull: a pictorial essay. Metastasis. Axial contrast-enhanced CT, with brain (a) and bone (b) windows showing a left parietal lytic, widely necrotic, lesion with intra- and extracranial extension. MRI better depicts extraosseous spread on both intra- and extracranial aspects, with dural displacement and thickening, better seen on coronal T2w image (c). The lesion presents diffusion restriction (d) and enhancement (e, f) of the peripheral solid component. T1w (e) and T1w after contrast administration with fat saturation (f) images

Imaging of
skull vault tumors in adults. Miscellany. Paget disease (a, b) CT (a) and X-ray (b): Characteristic mixed bone lysis and sclerosis, cortical bone thickening, and expansion. Osteoporosis circumscripta cranii CT (c, d): large geographic radiolucent areas involving medullar and cortical bone in frontal and occipital regions (arrows). Amyloidoma (e, f) CT (e) and T2WI (f): Giant heterogeneous mass with marked T2 hypointensity and calcifications. Renal osteodystrophy CT (g): shows characteristic “salt-and-pepper pattern.” Brown tumor (h, i): unspecific well-defined, cystic appearance (arrows). Thalassemia CT (j): Diffuse diploic widening and “hair-on-end” appearance (arrow) with characteristic occipital bone preservation (arrowhead). Bone sarcoidosis (k, l) CT (k) and T2WI (l): Mixed predominantly lytic multiple lesions with lace-like internal pattern of calcification and T2 hypointensity (dashed arrows). Osteitis CT (m, n): Bone focal lysis and erosions of osteitis (arrows) contiguous to a frontal sinusitis complicated with intracranial laminar abscess (dashed arrow)
Lytic skull lesions have a relatively wide differential that can be narrowed, by considering if there are more than one lesion and whether the mandible is involved.
Pathology
Causes
- lytic skeletal metastases
- multiple myeloma
- epidermoid - scalloped border with a sclerotic rim
- eosinophilic granuloma - Langerhans cell histiocytosis
- hemangioma
- Paget disease (osteolytic phase)
- osteomyelitis
- plasmacytoma
- lacunar skull (craniolacunae, Lückenschädel)
- pacchionian granulation
- vascular markings
- sarcoidosis
- burr hole craniotomy
- calvarial doughnut lesion
Mnemonic: MEL TORME
Siehe auch:
- Tumoren der Schädelkalotte
- Läsionen der Schädelkalotte
- Hämangiom Schädelkalotte
- Osteomyelitis
- osteolytische Knochenmetastasen
- Lipom der Schädelkalotte
- Multiples Myelom
- Knochenmetastasen des Schädels
- Morbus Paget der Kalotte
- Histiozytose X
- renale Osteodystrophie Schädelkalotte
- eosinophiles Granulom des Schädels
- Epidermoid
- Epidermoidzyste der Kalotte
- Aneurysmatische Knochenzyste des Schädelknochens
- intraosseous lipoma of the parietal bone
- Riesenzelltumor des Schädelknochens
- MEL TORME
und weiter:


 Assoziationen und Differentialdiagnosen zu Osteolysen der Kalotte:
Assoziationen und Differentialdiagnosen zu Osteolysen der Kalotte: